Rectal cancer ranks 6-7 in frequency among other localizations, accounting for about 4-5% of all cancers. Among localizations in the intestine, rectal cancer ranks first (70-80% of all types of intestinal cancer).
Since rectal cancer usually develops against the background of a previous chronic precancerous disease , its symptoms, especially early ones, are often nonspecific and no different from what the patient had to deal with before. That is why people with chronic intestinal pathology, as well as those who are at risk for this disease due to other parameters, should undergo regular medical examinations in order not to miss the onset of the development of a malignant tumor that requires cancer treatment abroad.
Spread of rectal tumor
A rectal tumor “kills” quite slowly. The neoplasm grows around the circumference of the intestine for a long time, moving from bottom to top.
It takes 1.5 – 2 years for complete destruction of the tumor organ.
Next, the tumor extends beyond the walls and lumens of the rectum, making its way to the tissue, finally affecting neighboring organs.
Cancer cells move throughout the body using lymph and blood, and metastases (new foci of cancer) are formed.
This type of cancer is characterized by metastases in the lungs, liver, and adjacent lymph nodes.
It is difficult to determine a malignant tumor on your own; in most cases, it is recognized during an appointment with a specialist.
There are only signs of a rectal tumor:
- Mucus or blood is secreted in the anus;
- Disturbed stool, alternating constipation and diarrhea;
- Sharp pain is felt in the rectum;
- Defecation is accompanied by pain, frequent urge to defecate.
These symptoms simply make it clear that the problem is in the rectum, not necessarily a manifestation of cancer.
X-ray examination
X-ray examination has also not lost its importance in the diagnosis of rectal cancer, although at various times opinions have been expressed about its uselessness due to the fact that the rectum is accessible to digital and endoscopic examination.
This study is indicated to clarify the diagnosis and the nature of the local spread of the tumor (Melnikov R.A., 1983; Arablinsky V.M. et al., 1984). In addition, an important task is to obtain information about the anatomical features and condition of the sigmoid and other parts of the colon. Taking into account the deep location of the rectum, its anatomical bends in different planes, and the need for a separate study of the colon, the X-ray examination technique is labor-intensive and requires the use of special techniques.
Preparing the patient for the study is essential. We use the following preparation method. If there is constipation, the patient is prescribed 30.0 g of castor oil within 15-16 hours. The evening before the study, two cleansing enemas “to clean water” are prescribed with an interval of 30-45 minutes. The patient does not have dinner or breakfast, and 1.5-2 hours before the study, two cleansing enemas are repeated with an interval of 30 minutes.
There are several methods for conducting the study itself: the method of partial filling of the distal parts of the intestine, the method of simultaneous examination of the rectum and colon, the parietography method, the polypositional method, etc.
The most widely used method is the simultaneous examination of the rectum and colon. As with other techniques, a barium suspension is used as a contrast agent at the rate of 1 part barium sulfate to 4 parts water with the addition of tannin (5-10 g per 1 liter).
Using special rubber tips or tubes, a contrast mass is injected using a Janet syringe or using a Bobrov apparatus. Often, due to the presence of sphincter incompetence and the need for rapid, isolated filling of the rectum, special obturators are used.
During the process of filling the rectum and colon, survey and targeted radiographs are taken in the optimal positions of the patient. If necessary, palpation compression of various parts of the intestine should be used. After the study with tight filling of the rectum, the patient empties the intestines and the second stage of the study is performed - double contrasting of the intestine. To do this, it is inflated with ordinary air. Against the background of double contrast, a detailed study of the relief of the mucous membrane becomes possible.
In order to study the local prevalence of rectal cancer detected during irrigoscopy, it is advisable to perform parietography in a number of patients after 2-3 days. It consists of studying a distended rectum under conditions of pneumoperitoneum. Studies include tomography: 1-2 slices in a frontal projection at a depth of 4-12 cm and 1-2 slices in a lateral projection.
X-ray signs of rectal cancer
Radiological signs of rectal cancer are studied on radiographs.
Conventionally, they can be divided into main and secondary or indirect. The main radiological signs of rectal cancer are: filling defect, pathological restructuring of the relief of the mucous membrane, additional shadow against the background of air. A filling defect is detected when filling is tight and is most often marginal; less often it has a central location. The shape, size, and boundaries of the defect are determined by the growth pattern, size, and location of the tumor. These signs are most clear in exophytic tumors. A filling defect in rectal cancer is characterized by a predominance of the width of the base of the tumor over the height, uneven and unclear contours, a distinct border with unchanged walls, and an asymmetric narrowing of the intestinal lumen (Fig. 25.1).
Rice. 25.1. X-ray of the rectum. Patient I. 67 years old. Rectal cancer stage III
Disturbances in the relief of the mucous membrane are detected at the double contrast stage. These disorders are manifested by a disordered structure of the folds of the mucous membrane, the presence of irregularly shaped defects, and contrast depots. Breaks of folds are detected, a symptom of a ring bordering an exophytic tumor (Fig. 25.2).
Rice. 25.2. X-ray of the rectum. Patient M., 64 years old, stage III rectal cancer
An additional shadow of the tumor, detected at the stage of double contrast, corresponds to the location of the filling defect. It usually has an irregular shape and uneven contours. In its center, clearing is sometimes detected as a sign of tumor ulceration. The boundaries of the shadow can be sharp or with a gradual transition into an unchanged wall during its cancerous infiltration (Fig. 25.3).
Rice. 25.3. X-ray of the rectum. Patient I. 67 years old. Rectal cancer stage III
Secondary or indirect radiological signs are: persistent depots of barium suspension after bowel movement; expansion of the intestine above and below the area affected by the tumor; shortening and deformation of the intestine; incomplete evacuation of barium suspension after bowel movement; rigidity of the walls of the rectum; expansion of the rectal ampulla, delay in the advancement of contrast at the lower pole of the tumor during retrograde filling; thinning or widening and rigidity of the folds of the mucous membrane; signs of colonic obstruction.
Some radiological symptoms of rectal cancer, which are of a variable nature, are also described: the “hourglass” symptom; reduction in the size of the rectum; uneven expansion of the retro-rectal space; fixation of one or another section of the intestine when the tumor grows into the perirectal tissue.
Auxiliary symptoms have diagnostic value in cases where there is a combination of at least 2-3 symptoms.
The X-ray method is a reliable and informative research method. With its help, you can confirm and supplement information about the nature of the tumor, its location and local prevalence.
In addition, you can obtain comprehensive information about the condition of the entire colon and identify the presence of multiple primary tumors. X-ray examination was performed in 201 patients (90.0%). In 20 patients, it turned out to be impossible due to complete obstruction of the lower ampullary or anal parts of the rectum. We did not encounter any diagnostic errors during X-ray examination in patients with rectal cancer. However, such errors are possible. They are especially often allowed for cancer of the supramullary region.
In addition, the capabilities of irrigoscopy are limited in obtaining reliable information about the nature and extent of local spread of the tumor to surrounding organs and tissues, and about possible damage to regional lymph nodes by metastases.
Possible invasion of rectal cancer into the ureter, bladder, seminal vesicles and vas deferens can be detected by X-ray examination of these organs. It should begin with excretory urography. In case of compression of the ureter, there is a violation of the passage of urine from the upper urinary tract, and hydroureteronephrosis occurs.
A descending cystogram reveals a filling defect, deformation or asymmetry of the bladder due to its growth by a tumor. An ascending cystogram can more clearly reveal invasion of the bladder wall. A classic sign is asymmetry of the bladder shadow and a filling defect with uneven, pitted contours.
The growth of rectal cancer into the seminal vesicles and vas deferens can be detected by vesiculography. There are ascending and descending vesiculography. Ascending vesiculography is performed after the introduction of a radiopaque substance into the vas deferens during transurethral catheterization.
Descending vesiculography is performed by direct puncture or vasotomy of the vas deferens through an incision in the scrotum. The most characteristic signs indicating the involvement of the vas deferens in the tumor process are defects in the filling of the seminal vesicles, discontinuity of their contours up to complete amputation, and impaired patency for the contrast agent. A number of authors attach a certain importance to angiography, considering it an important additional method for determining the extent of the tumor.
The experience of using selective lower mesentericography in patients with rectal cancer allowed V.N. Berdov et al. (1986) not only confirm the presence of a tumor, but also determine the depth of infiltration, while differentiating germination to the submucosal layer, to the muscular layer of the intestinal walls and damage to all layers. These authors established the diagnostic value of various angiographic signs of rectal cancer (Table 25.1).
Table 25.1. Hagiographic signs of intramural spread and extraorgan growth of rectal cancer (Berdov V.I., Tsyb A.F., Yurchenko I.I., 1986)
| No. | Signs | Correlation coefficient |
| Intramural spread | ||
| 1 | Pathological vessels in the thickness of the wall and projectionally in the intestinal lumen | +0.834 |
| 2 | Slight thickening of the intestinal wall at the level of the tumor | +0.832 |
| 3 | Clarity of the contours of the intestinal wall at the base of the neoplasm | +0.815 |
| 4 | No changes in the architecture of the veins of the rectal tissue | +0.449 |
| 5 | Venous outflow for 8-12 seconds | +0.226 |
| 6 | Weak venous outflow from the tumor focus | +0.138 |
| Extraorganic growth | ||
| 1 | Pathological vessels outside the intestinal wall | +0.884 |
| 2 | Accumulation of contrast agent outside the organ | +0.882 |
| 3 | Blurred outline of the intestinal wall at the base of the tumor | +0.815 |
| 4 | Deformation of the venous vessels of the rectal plexus and the main trunk of the superior rectal vein | +0.446 |
| 5 | Deformation of large arterial branches (1-2 orders of magnitude) | +0.434 |
| 6 | Early venous drainage | +0.266 |
| 7 | Intense venous outflow from the lesion | +0.134 |
In some cases, angiography can detect metastases in the lymph nodes.
Additional information about the depth of infiltrative growth of rectal cancer can be obtained using pelvic arteriography. At the same time, there is a point of view that arteriography for rectal cancer is uninformative and does not determine subsequent treatment tactics, and the traumatic nature and existing dangers limit the indications for its use. In any case, this method is not widely used in clinical practice.
Stages of the disease
- Stage I - the tumor size is approximately 2 cm, extends to the submucosal and mucous layers. There is no damage to the lymph nodes yet. Regional metastases are not observed.
- Stage II - an ulcerative or ordinary tumor is 5 cm in size, but does not extend beyond the outer muscular layer.
- Stage III - the tumor has a larger diameter, spreads to the layers of the intestinal walls, fatty tissue may be affected.
- Stage IV - a large tumor does not move, distant metastases spread to neighboring organs.
Diagnosis of rectal tumors
For rectal cancer, there are the following diagnostic methods:
- Physical examination, a specialist during diagnosis evaluates: the condition of the skin (it has a pale color), changes in body weight (the person is losing weight), the abdomen may be swollen, the presence of palpation of the inguinal lymph nodes and liver.
- Endoscopic examination. Using sigmoidoscopy, you can visually assess the condition of the neoplasm, the size and intensity of its extent and the lower edge. For morphological analysis, a tumor biopsy is performed.
- Ultrasound examination, computed tomography of the intestines and organs, x-ray examination, this is how the spread of the tumor process is clarified.
Clinical manifestations of the disease
It is very difficult to identify the disease at an early stage, due to the lack of characteristic signs and symptoms characteristic of intestinal cancer.
The following signs should be a reason for concern and a visit to a therapist, proctologist, or :
- Painful sensations in the right or left half of the abdomen;
- Unmotivated weight loss;
- Nausea, vomiting;
- Feeling of heaviness and fullness in the abdomen even after a bowel movement;
- Frequent intestinal disorders: flatulence, diarrhea, constipation.
The first signs of intestinal cancer are washed away and are often confused with other diseases of the digestive tract. The patient's complaints and the above symptoms must be supplemented with appropriate tests and diagnostic examinations.
Timely actions will help to recognize the manifestation of the disease at an early, first stage, which in the future can give a positive treatment result.
The intestine is divided into two segments: thin and thick, which in turn include other sections. Cancer affects in most cases the small intestine, colon, and rectum. The disease manifests itself differently in different places in the intestine, so it is advisable to consider its first manifestations, symptoms and signs individually.
Signs of small intestine cancer
Tumors in the small intestine can be benign or malignant and are less common than in the large intestine. The first signs of advanced cancer are:
- Anemia;
- Unreasonable weight loss;
- Weakness, apathy;
- Intestinal bleeding;
In the absence of specific symptoms and signs characteristic of small intestinal cancer, detection of the disease at an early stage is achievable exclusively through instrumental examinations.
Symptoms of Colon Cancer
The manifestation of colon cancer is determined by the location of the tumor, size, and aggravation of the condition. The first signs of early cancer are:
- Discomfort in the intestines - manifested by a feeling of heaviness, lightheadedness, belching.
- Many cancer patients experience symptoms such as bloody, purulent discharge.
- High temperature, weakness, anemia are symptoms and signs of a malfunction in the patient’s general well-being caused by intoxication.
- At an early stage, pain in the abdominal area is nagging and aching. The progression of the disease brings cramping, intense pain, indicating complete or partial movement of contents through the intestines.
- An intestinal disorder manifests itself by alternating diarrhea with constipation, flatulence, and severe abdominal distension.
Symptoms of colon cancer are divided into six forms:
- Symptoms of toxic-anemic form.
The first signs of this form of cancer are: excessive fatigue, body temperature stays within 37-37.5 ºС, dullness of the skin, anemia. Anemia indicates that cancer is growing rapidly.
- The form is enterocolitic.
This form of cancer is similar in its symptoms to inflammatory and infectious diseases of the gastrointestinal tract. It manifests itself as obvious intestinal disorders: bloating, turbulence in the abdomen, difficulty in bowel movements, diarrhea. The nature of the pain is aching. Feces contain blood and mucus.
- Symptoms of dyspeptic form.
Symptoms of this form are not characteristic of cancer; they are observed as signs of many other gastrointestinal diseases. With dyspeptic cancer, the upper abdomen hurts, nausea, vomiting, bloating in the stomach area, and loss of appetite are pronounced.
- Obstructive.
The first and main sign of the obstructive form of cancer is intestinal obstruction, which is expressed by the irregular occurrence of the following symptoms: difficulty passing gases and feces, paroxysmal pain, a feeling of fullness in the abdomen.
- Pseudo-inflammatory.
The form of cancer manifests itself with abdominal pain and fever. Such a common symptom as intestinal disorders is mild.
- Tumor-like form.
A characteristic feature of this form is absent or mild symptoms and signs. During a medical examination and diagnostic testing, cancer can be detected.
Symptoms of rectal cancer
The first significant symptoms of the disease appear when the tumor has reached a large size. The severity of rectal cancer is determined by the location, size of the tumor, and the level of development of the disease:
- Painful sensations with cancer are continuous, but this is not an early sign of the disease; on the contrary, such a symptom indicates the spread of the tumor and damage to adjacent organs and tissues.
- An irreversible symptom is discharge from the anus during bowel movements. Feces mixed with dark blood indicate the fact that the tumor was injured by feces. The progressive development of cancer is determined by purulent, mucous discharge. This symptom indicates the beginning of the disintegration of the neoplasm, an infectious inflammation.
- Early signs of rectal cancer are intestinal disorders, alternating diarrhea with constipation and vice versa. Tenesmus often occurs - the urge to defecate, which does not have a positive result. Instead of feces, only blood or mucus may be released.
- The shape of stool for rectal cancer is ribbon-like, which is the first sign of this disease.
- The growth of a cancerous tumor narrows the space of the intestine, then signs of intestinal obstruction appear: sharp pain, constipation, inability to pass gas, bloating, nausea.
- Common symptoms of rectal cancer are: hyperthermia, gradual anemia, impotence, weight loss.
Causes of rectal tumor
The causes of rectal tumors have not yet been fully established.
There are only a few risk factors that increase your chances of getting cancer.
- Poor nutrition. If the diet does not contain foods with sufficient fiber, a tumor may form, initially benign. High-calorie foods slow down bowel movement. This leads to the fact that the process of nutrients entering the human body slows down; they do not reach the intestine. Vegetarians suffer from colorectal cancer much less frequently.
- Contact with certain poisons, especially asbestos.
- Chronic or acquired diseases of the organ, inflammatory processes, as well as polyps.
- Anal sex and human papillomavirus infection. Not long ago, scientists found that passive homosexuals, in whom the virus predominates, are more likely to develop colorectal cancer.
Intestinal polyps
Intestinal polyposis is the main oncogenic disease.
- Their malignancy is high, and the tumor quickly becomes malignant.
- The intestines can transform into cancer even with single polyps.
- The chance of cancer spreading with familial polyps increases.
Colonoscopy helps determine the primary form of polyps: when observing villous adenomas, the tumor develops into malignant in approximately 40% of cases. And for tubular adenomas – 2-6%.
Is it possible to detect colorectal cancer?
The length of the rectum is about 20 cm, this is the final section in the large intestine, in this place the digestive processes are completed and the formation of feces begins.
The rectum has several parts (anatomical areas), they differ in structure and embryonic origin, in each area the cancer behaves differently, making it easier for specialists to diagnose the stage and level of the lesion.
In total, there are three parts in the anal colon: the perineal part, its length does not exceed 3 cm; in this area there are sphincter muscles responsible for the process of defecation.
The second part (middle) is ampullary, its length is no more than 1 cm, in this area the absorption of the bolus of food, namely its liquid part, begins to form feces.
The last part is supramullary, it has a peritoneum, no more than half a centimeter in length.
The localization of rectal tumors in 80% of cases occurs in the ampullary region; there is practically no localization in the anorectal region.
In the first case, the section is covered with glandular epithelium, which has one layer, the supramullary section most often affects glandular cancer - experts distinguish adenocarcinoma tumors of the rectum, there is another classification: solid cancer, mixed, signet ring cell, scirrhus, are affected in most cases.
The second section (anorectal) has multilayered epithelium, in this case squamous cell carcinoma and melanoma predominate.
The nature of the spread of metastases in the rectum can be determined by determining the anatomical features of the organ and the level of its blood supply.
Quite often, metastases spread their effects to the liver, this is explained by the peculiarities of the venous outflow emanating from the upper parts of the intestine; it passes into the portal vein system, part of the liver.
The lower parts of the rectum have a high level of blood supply, so the tumor can metastasize to the lungs, other organs, and affect organs, passing through the vena cava system.
Main stages of the disease
There are different approaches to dividing colorectal cancer into stages. The most common among them is the division of the disease in question into 5 stages (from 0 to 4).
Stage 0 or early rectal cancer
Low-quality neoplasms have scanty parameters and are localized in the epithelial layer of the rectum. The prognosis is favorable: 5-year survival rate after treatment of stage 0 of this type of cancer is 95-96%.
1 - first stage of rectal cancer
The neoplasm is not limited to the epithelial layer of the rectum: it extends beyond it without affecting the muscle tissue. The tumor parameters do not exceed 2 cm. It is easy to visualize during examination. Surgery + chemotherapy help cope with the disease in question at the first stage.
2 - second stage of rectal cancer
A malignant neoplasm affects all layers of the rectum (including muscle tissue). The tumor reaches 45-50 mm in size. Single metastases to the lymph nodes may occur. Five-year survival rates are possible at 55-80%.
3 - third stage of rectal cancer
The tumor occupies half/most of the diameter of the rectum (its parameters are from 5 cm). Cancer cells spread to the lymph nodes that are located near the intestines. Multiple metastases may occur. Based on the shape of the tumor and the protective abilities of the patient’s body, 5-year survival will be recorded in 20-50% of cases.
4 - fourth or last stage of rectal cancer and metastases
Cancer cells spread to nearby organs and disrupt their functioning. Metastases often occur in the liver, ovaries, and lungs. The prognosis is poor: the possibility of 5-year survival is less than 1%.
Recurrence of rectal cancer
Associated with incomplete elimination of the causes that caused the appearance of rectal cancer. As a result, the disease in question with all its manifestations re-develops. The average duration during which the disease can return is 13 months. Although in 15% of cases, relapse is recorded 2 years after surgical treatment of cancer.
Recurrence at the site of the removed tumor can occur as a result of certain factors.
- Rupture of the tumor during surgical procedures.
- Growth of the rudiments of a pathological formation: the tumor was not completely removed.
- Sedimentation of malignant cells in the area of the laparoscopic port.
Treating a relapse of this disease (like any other cancer) is more difficult than the initial pathology. The consequences may be more serious.
Often, treatment for relapse is not effective. This is due to several factors.
- Late diagnosis of recurrent rectal cancer. In some cases, the disease in question may be asymptomatic.
- Poor defense reactions of the body (consequence of chemotherapy treatment).
- Imperfect technique of operations that should be performed for recurrent rectal cancer.
Symptoms of a rectal tumor
After the diagnosis of a rectal tumor is established, the first symptoms begin to appear.
The onset of tumor damage is characterized by alternating loose stools and constipation, frequent false bowel movements (tenesmus) occur, similar to the manifestation of hemorrhoids, as discharge appears from the anus, this may be blood and pus.
A tumor grows near the intestinal walls, affecting the functioning of the corresponding nerves, which leads to painful sensations.
If the muscles that relate to the formation of the anal sphincters are affected, gases and feces are released involuntarily.
If we are talking about an oncological disease of the anorectal area, where there is impaired functioning of the rectal sphincter, then pain appears in the initial stages.
When the tumor affects the lumens of the rectum (exophytic cancer), as well as saucer-shaped tumors, tumors in the form of ulcers, the main manifestations of the disease are considered to be inflammatory processes, as well as bleeding in the early stages.
Blood is visible in most cases mixed with stool. At a later date, pus or mucus may appear parallel to the blood.
General health worsens, apathy, fatigue, dizziness, and frequent vomiting appear.
This occurs due to prolonged blood loss, which turns into tumor intoxication, and is observed closer to the later stages of the disease.
Urinary incontinence is also observed, as further enlargement of the tumor puts pressure on functioning organs.
Clinical diagnosis of cancer
To establish a diagnosis, the patient must undergo a series of tests: laboratory and instrumental. At an early stage, it is extremely difficult to identify the disease on your own; doctors recommend regular medical examinations. This will allow you to detect the onset of pathological processes and begin treatment without taking radical measures.
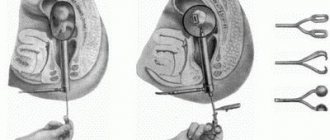
The doctor begins the diagnosis by asking about complaints and taking an anamnesis. If a patient’s direct relatives suffer from cancer, then the patient is at risk. Next, the doctor can conduct a digital examination of the rectum and examine it with speculum. During the examination, the doctor inserts the index finger into the patient's anus and palpates the intestinal mucosa for the presence of formations or polyps. The examination can also be carried out using a rectal mirror: the instrument expands the lumen of the rectum and increases the field of view.
The patient must undergo a general blood test.
Before making a diagnosis, the patient undergoes a number of tests, general and specific:
- general blood analysis;
- blood chemistry;
- blood test for tumor markers;
- urine test;
- coprogram;
Biopsy, histology and cytology
- A biopsy is the removal of a small amount of tumor tissue. After this procedure, the material is subjected to cytological or histological examination.
- Histology is the study of a tumor sample under a microscope. The analysis allows you to make an accurate diagnosis, determine the nature of the tumor and the degree of development of the disease.
- Cytology is the study of the cellular structure of a material. Both a tissue sample obtained from a biopsy and blood, pus or mucus taken from the rectum are suitable for cytology analysis.
Instrumental diagnostic methods
Depending on the patient’s condition, the doctor chooses a computer diagnostic method:
An ultrasound of the abdominal organs is done if it is impossible to undergo an MRI or CT scan.
- Ultrasound. Ultrasonography. Helps evaluate the condition of the lymph nodes and abdominal organs. It is considered the least reliable method of computer diagnostics and is performed in case of contraindications to CT and MRI.
- MRI. Magnetic resonance imaging. During the study, detailed visualization of the neoplasm is carried out: its size, the degree of invasion into neighboring organs. The need for surgical intervention is assessed. One of the most reliable diagnostic methods. MRI is contraindicated: if there is metal in the patient’s body or implants, pacemakers, titanium plates, etc.;
- in the first trimester of pregnancy;
- acute renal failure in the patient;
- contrast intolerance.
Colonoscopy
During the procedure, an endoscope is inserted into the patient's rectum. Colonoscopy allows you to view the entire large intestine for tumors, polyps, and other pathological conditions. During a colonoscopy, the doctor may take a biopsy to test the histology of the tumor, or remove intestinal lesions such as polyps or growths. Carrying out the operation in this way contributes to the patient’s rapid recovery by minimizing tissue damage that occurs during a full-fledged surgical intervention.
X-ray of the rectum
Irrigoscopy allows you to determine the main characteristics of the tumor.
X-ray examination of the rectum is called irrigoscopy. Contrast is injected into the rectum and a series of pictures are taken. X-ray evaluates the location of the tumor, the degree of ingrowth, the direction of growth (inward or outward), and the presence of ulcers on the intestinal wall. This procedure is contraindicated for frail and elderly patients.
Differential diagnosis
The differential diagnosis of rectal cancer is aimed at excluding other variants of proctological diseases, including hemorrhoids. Hemorrhoids and rectal cancer have quite similar external manifestations. Considering the external manifestations of these diseases, it seems that the symptoms are the same, but this is not so. When bleeding caused by hemorrhoids, the blood is always scarlet in color and can be easily seen in the patient's stool.
In the case of rectal cancer, the blood may be very dark (if the tumor is located high up) and mixed with the stool. Often its presence can only be verified through analysis. A patient suffering from cancer rapidly loses weight; with hemorrhoids, this symptom is absent. In general, the diagnosis of hemorrhoids includes a number of studies. Digital examination, colonoscopy, rectoscopy, x-ray and biopsy give the doctor the opportunity to make a differential diagnosis of hemorrhoids.
Rectal surgery
There are 4 types of surgery to remove a rectal tumor, depending on the site of spread and stage of the disease: intra-abdominal rectal resection or anterior resection, low rectal resection (anterior), Hartmann's surgery, and rectal extirpation.
In the case when the tumor has spread and affected the upper third of the organ, intra-abdominal anterior resection of the rectum is prescribed, which helps in the initial and middle stages.
Anterior resection is the removal of the tumor-affected intestine, its ends are sutured.
Basically, stitching is done manually so as not to miss details, but special equipment can be used.
The sphincter is preserved during intra-abdominal surgery; only the affected area is removed.
The results after this type of surgery are the most successful, but it is worth noting that such an operation is not always possible due to the peculiarities of human anatomy, as well as the large size of the tumor.
The Hartmann method completely removes the tumor in the rectum; the operation removes the upper part (end) of the intestine as a colostomy, and sutures the lower part.
This operation is prescribed when there is an increased risk of stitching the ends of the intestine. If the operation is repeated, the colostomy can be removed.
Causes
Malignant and benign tumors located in the rectum are formed under the influence of approximately the same factors:
- presence of illness in close relatives;
- nature of work;
- bad habits;
- one-sided nature of nutrition;
- other intestinal diseases;
- excess weight;
- hypovitaminosis;
- age over 60 years;
- immunosuppressive conditions;
- constipation.
If a malignant process was observed in parents or in another generation, then the person is at risk for oncology. Working in a workshop with harmful emissions, the nature of activities with heavy metals, toxic gases also contribute to the development of abnormal phenomena.
A tumor in the rectum can form if a person drinks or smokes, especially in cases where the quality of the product is low. Cigarettes contain dozens of carcinogenic substances, which has been confirmed by research. Alcohol is transformed in the liver, but passes through the entire digestive tract. It disrupts the activity of the enzymatic system, dulls the reaction rate, poisons the brain, and damages sensitive cells.
Human nutrition must contain the main groups of substances, for which the diet is made up of vegetables and fruits, cereals, meat and dairy products. From each of these categories the body draws a source of energy. In addition, plant foods are a source of fiber, which has a soluble and insoluble part, due to which the digestive tract is “cleansed” of excess. If a person does not eat vegetables and fruits, the intestines become filled with waste, the excess is not excreted, which damages its walls. Tumors of the rectum and other parts become the result of this process.
Chronic constipation, which occurs due to a malignant process, is associated with a predominance of meat in the diet, especially pork and beef.
A healthy organ that receives a balanced diet cannot get sick. The presence of damage in the form of anal fissures and hemorrhoids, as well as colitis (inflammation of the mucous membrane) are favorable conditions for cell transformation.
Crohn's disease is a precancerous disease that combines several symptoms. It affects the small intestine and the beginning of the large intestine, but affects all parts of the structure. The essence of chronic inflammation is the presence of inflammation of the small or large intestine, which penetrates into the deep layers of the wall, forming ulcers. Leukocytes accumulate around the erosions, forming infiltrates. When the elements heal, rough scars form. Cancer cells can divide in this tissue.
Antioxidants are designed to neutralize substances that cause cancer. If they enter the body in short supply, the protection is weakened. With a sedentary lifestyle and obesity, the risk of tumor increases.
We recommend reading Ewing's Sarcoma - what kind of disease it is, survival rate, types
The occurrence of rectal oncology is influenced by a decrease in immunity; it develops due to a deficiency in the synthesis of lymphocytes and natural killer cells, which are responsible for the fight against tumor cells.
Treatment of rectal tumors with radiation therapy and chemotherapy
Radiation diagnostics and treatment are used in parallel with chemotherapy, as well as as a completion after surgical treatment.
Radiation therapy reduces the diameter of the tumor, thereby simplifying removal; colostomies can be avoided, and there is a risk of relapse.
Tumor metastases are treated and also prevented using chemotherapy.
It has been scientifically proven that chemotherapy stops the spread of cancer to other organs, thereby increasing the patient's life expectancy.
Chemotherapy is carried out every six months for this diagnosis, but the timing depends on the speed of spread of metastases.
In the first stages, only radiation and chemotherapy without surgery are sufficient.
Complications
With further stages of the disease, complications may occur:
- the tumor will grow onto the walls of the pelvis and also spread to neighboring organs;
- pus and inflammatory processes appear in the area of the tumor;
- bleeding begins in the rectum;
- intestinal obstruction.
Rectal cancer often metastasizes through the blood and lymphatic vessels.
The pelvis is most often affected. But this happens due to late presentation to the hospital.
If you have the slightest suspicion about the presence of a tumor (even benign), contact a specialist immediately.
You will be prescribed the necessary procedures, ultrasound, diagnostics, which will determine whether you have cancer.
If rectal polyps or cancer have already been observed in the family, prevention should be carried out every year.
Phlebography
Phlebography has become much more common.
The successful development of pelvic phlebography began with the well-known works of Dos Santos (1938), who substantiated its use in the diagnosis of various diseases. The basis for the development of pelvic phlebography was laid by the studies of the anatomist Batson (1940, 1942), the results of which were then confirmed by other authors. In 1950, De la Pena obtained x-ray images of the pelvic veins in humans. A variety of contrast agent injection methods have been proposed to obtain this image.
It was injected into the veins of the penis; corpora cavernosa of the penis in men and the clitoris in women; delirious vein; great saphenous vein of the thigh; simultaneously into several venous vessels; into the uterus.
Due to a number of disadvantages of these phlebography methods associated with unclear contrast of the pelvic veins, difficulties in interpreting fistograms due to rapid evacuation of contrast, and the possibility of complications, attention was paid to the method of intraosseous administration of a contrast agent, which turned out to be optimal.
Pelvic venography has become widely used in the diagnosis of tumors of the prostate gland and bladder; tumors of the uterus, ovaries. The high informativeness of pelvic venography in determining the nature and degree of local prevalence of malignant tumors of the pelvic organs has been proven. In order to study the diagnostic capabilities of pelvic phlebography in the diagnosis of rectal cancer, one of us undertook a special study [Yaitsky N.A., 1968].
Pelvic venography performed in patients with rectal cancer revealed a variety of radiological symptoms. The most characteristic changes in phlebograms are: disruption of the contours of the veins (Fig. 25.4); the presence of crescent-shaped defects in the filling of veins (Fig. 25.5); retrograde flow of contrast agent; filling of collaterals and anastomoses (Fig. 25.6); varicose veins (Fig. 25.7); partial or complete block of venous blood flow and displacement of veins (Fig. 25.8).
Rice. 25.4. Intraosseous pelvic venogram Patient B., 61 years old, stage III rectal cancer. Sharp deformation and inward displacement of the left external iliac vein
Rice. 25.5. Intraosseous pelvic venogram Patient P., 64, stage III rectal cancer. Crescent defects in the filling of both hypogastric veins
Rice. 25.6. Intraosseous pelvic venogram Patient A. 58 years old. Rectal cancer stage IV. Abundance of anastomoses and collateral flow
Rice. 25.7. Intraosseous pelvic venogram. Patient B., 52 years old. Cancer of the proctosigmoid region, stage IV. Dilatation of the veins of the left half of the pelvis. Crescent defect of the right hypogastric vein
Figure 25.8. Intraosseous pelvic venogram. Patient 3. 52 g. Cancer of the upper ampullary rectum. Block of venous blood flow due to tumor compression of the common iliac veins
The most common symptom was a symptom of a violation of the venous contour (in 49.4% of patients). This sign is pathognomonic for paravasal metastasis. Crescent defects—multiple and single—were observed in 41% of patients. Multiple and, especially, bilateral crescent-shaped defects in the filling of veins indicate multiple metastases to the pelvic lymph nodes.
With the help of intraosseous pelvic venography, it is possible to identify changes in the veins that are not associated with metastases, but directly with the tumor itself. These changes most often occur in the form of compression and germination of the venous trunks of the pelvis by the tumor (Fig. 25.9).
Rice. 25.9. Intraosseous pelvic venogram. Patient G. 39 years old. Stage III rectosigmoid cancer. Tumor invasion of the right internal iliac vein
Similar changes were detected in 13.6% of patients. When a tumor or its large metastases compress or invade veins, a complete or partial block of venous blood flow usually occurs (Fig. 25.10). More often it happens on one side, less often - bilateral.
Rice. 25.10. Intraosseous pelvic venogram Patient G. 25 years old. Recurrence of sigmoid colon cancer. The arrow indicates the place of compression of the common iliac veins by a recurrent tumor
X-ray symptoms of invasion of vein walls are quite peculiar. In the initial stages of germination, the wall of the vein is as if eaten away in the form of saw teeth (Fig. 25.11). With more massive germination, amputation of veins is observed (Fig. 25.12).
Rice. 25.11. Intraosseous pelvic venogram. Multiple filling defects of the right hypogastric vein and left common iliac vein
Rice. 25.12. Intraosseous pelvic venogram. Patient K, 90 years old. Rectal cancer stage IV. Amputation of both internal iliac veins of the left obturator vein and veins of the sacral plexus
The interpretation of pelvic phlebograms is greatly facilitated if seriograms are performed, which make it possible to dynamically track the flow of contrast agent into the pelvic veins. The pelvic venography method is of particular value in cases of detecting relapses and metastases after previously performed surgical interventions.