A disease such as mitral valve prolapse, the treatment of which can be either conservative or surgical, or not prescribed at all (depending on the form of the disease), is the most common anomaly of the heart valves. Often it is not dangerous and is detected by chance during cardiac echocardiography (ultrasound examination). This diagnostic method is the most effective, as it allows you to determine the degree of the disease and the volume of blood return (regurgitation).
To understand the picture, it is important to know what a heart valve is. The heart functions as a pump in the body, ensuring blood circulation through it. This occurs by maintaining the required pressure in the chambers of the heart. There are four chambers in total - 2 atria and 2 ventricles. Valves are special dampers located between the chambers. They regulate pressure and set blood flow in the desired direction. There are four such valves in total.
Mitral valve prolapse is the abnormal protrusion of the valve leaflets as they close when the heart contracts. As a result, the valves do not close tightly, and part of the blood returns back - from the ventricle to the atrium or from the arteries to the ventricles.
What it is?
Left valve prolapse, or mitral valve prolapse, or bicuspid valve prolapse (BVP) is a disease accompanied by dysfunction of the valve located between the left atrium and the ventricle.
Normally, when the atrium contracts, the valve opens and blood flows into the ventricle. The valve then closes and the ventricle contracts, releasing blood into the aorta. With some pathology of connective tissue or changes in the heart muscle, a disturbance in the structure of the mitral valve occurs, which leads to “bending” of its valves into the cavity of the left atrium during contraction of the left ventricle, and part of the blood flows back into the atrium. The severity of this pathology is judged by the magnitude of the reverse flow.
It is believed that this disorder is most often observed in young people, but data from the Framingham study showed that there is no significant difference in the incidence of this disease depending on gender and in different age groups. In the case of a small return of blood (regurgitation), it is not clinically felt and does not require treatment. In rare cases, the amount of reverse blood flow is large and correction of the defect is required, including surgical intervention.
Anatomy
The heart can be imagined as a kind of pump that forces blood to circulate through the vessels of the whole body. This movement of fluid becomes possible by maintaining the pressure in the cavity of the heart and the work of the muscular apparatus of the organ at the proper level. The human heart consists of four cavities called chambers (two ventricles and two atria). The chambers are limited from each other by special “doors”, or valves, each of which consists of two or three doors. Thanks to this anatomical structure of the main motor of the human body, every cell of the human body is supplied with oxygen and nutrients.
There are four valves in the heart:
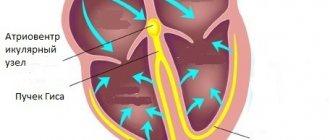
- Mitral. It separates the cavity of the left atrium and the ventricle and consists of two valves - anterior and posterior. Prolapse of the anterior valve leaflet is much more common than the posterior one. Special threads called chords are attached to each of the valves. They provide contact between the valve and muscle fibers, which are called papillary or papillary muscles. For the full functioning of this anatomical formation, the joint coordinated work of all components is necessary. During cardiac contraction - systole - the cavity of the muscular cardiac ventricle decreases, and accordingly the pressure in it increases. In this case, the papillary muscles are activated, which close the exit of blood back into the left atrium, from where it flows out of the pulmonary circulation, enriched with oxygen, and, accordingly, the blood enters the aorta and then, through arterial vessels, is delivered to all organs and tissues.
- Tricuspid (three-leaf) valve. It consists of three doors. Located between the right atrium and ventricle.
- Aortic valve. As described above, it is located between the left ventricle and the aorta and does not allow blood to return to the left ventricle. During systole, it opens, releasing arterial blood into the aorta under high pressure, and during diastole, it is closed, preventing blood from flowing back to the heart.
- Pulmonary valve. It is located between the right ventricle and the pulmonary artery. Similar to the aortic valve, it prevents blood from returning to the heart (right ventricle) during diastole.
Normally, the work of the heart can be represented as follows. In the lungs, the blood is enriched with oxygen and enters the heart, or rather its left atrium (it has thin muscle walls and is only a “reservoir”). From the left atrium it pours into the left ventricle (represented by a “powerful muscle” capable of pushing out the entire incoming volume of blood), from where during systole it spreads through the aorta to all organs of the systemic circulation (liver, brain, limbs and others). Having transferred oxygen to the cells, the blood takes up carbon dioxide and returns to the heart, this time to the right atrium. From its cavity, fluid enters the right ventricle and, during systole, is expelled into the pulmonary artery and then into the lungs (pulmonary circulation). The cycle repeats.
What is prolapse and why is it dangerous? This is a state of inadequate functioning of the valve apparatus, in which, during muscle contraction, the blood outflow pathways are not completely closed, and, therefore, part of the blood returns back to the heart during systole. So, with mitral valve prolapse, the fluid during systole partially enters the aorta, and partially from the ventricle is pushed back into the atrium. This return of blood is called regurgitation. Usually, with pathology of the mitral valve, the changes are insignificant, so this condition is often considered as a normal variant.
When is the surgical method used?
Surgical approaches can be of two types:
- fixation of torn valves (suturing of threads-chords, creation of a mechanism for holding the valves);
- replacement of the valve with an artificial prosthesis.
Indications for surgical treatment:
- unsuccessful therapy of endocarditis with antibiotics and various anti-inflammatory drugs;
- circulatory failure stage 2B, inability to use or lack of results from the use of cardiac glycosides, diuretics;
- repeated attacks of atrial fibrillation;
- development of hypertension in the pulmonary artery.
An artificial mitral valve is sewn in with a ring to prevent scarring of the opening between the atrium and ventricle
There are standard indicators of circulatory disorders that doctors rely on when deciding whether surgery is advisable:
- regurgitation flow more than 50%;
- residual emission fraction less than 40%;
- increase in pressure in the pulmonary artery more than 25 mm Hg;
- an increase in the volume of the left ventricular cavity during diastolic relaxation by 2 times or more.
Classification
Mitral valve prolapse can be:
- Primary. Associated with connective tissue weakness, which occurs with congenital connective tissue diseases and is often transmitted genetically. With this form of pathology, the mitral valve leaflets are stretched, and the retaining leaflets of the chord are lengthened. As a result of these violations, when the valve closes, the flaps protrude and cannot close tightly. Congenital prolapse in most cases does not affect the functioning of the heart, but is often combined with vegetative-vascular dystonia - the cause of symptoms that patients associate with heart pathology (periodically occurring functional pain in the chest, cardiac arrhythmias).
- Secondary (acquired). Develops in various heart diseases that cause disruption of the structure of the valve leaflets or chords. In many cases, prolapse is provoked by rheumatic heart disease (an inflammatory disease of the connective tissue of an infectious-allergic nature), undifferentiated connective tissue dysplasia, Ehlers-Danlos and Marfan diseases (genetic diseases), etc. In the secondary form of mitral valve prolapse, pain that passes after taking nitroglycerin is observed, interruptions in heart function, shortness of breath after exercise and other symptoms. If the cardiac chords rupture as a result of a chest injury, emergency medical attention is required (the rupture is accompanied by a cough, during which foamy pink sputum is released).
Primary prolapse, depending on the presence/absence of noise during auscultation, is divided into:
- The “silent” form, in which symptoms are absent or scanty, and noises and “clicks” typical for prolapse are not heard. Detected only by echocardiography.
- Auscultatory form, which, when auscultated, is manifested by characteristic auscultatory and phonocardiographic “clicks” and noises.
Depending on the severity of the sagging of the valves, mitral valve prolapse is distinguished:
- I degree - the doors bend by 3-6 mm;
- II degree - there is a deflection of up to 9 mm;
- III degree - the sashes bend by more than 9 mm.
The presence of regurgitation and the degree of its severity are taken into account separately:
- I degree – regurgitation is mild;
- II degree – moderately severe regurgitation is observed;
- III degree - there is pronounced regurgitation;
- IV degree – regurgitation is severe.
Reasons for development
Mitral valve prolapse is not an independent disease. It is a syndrome that occurs in numerous diseases. Depending on the etiology, secondary MVP is distinguished - it occurs as a result of other pathologies, and primary - it is also congenital or idiopathic.
Quite often, idiopathic MVP is detected in children and adolescents. It appears due to congenital connective tissue dysplasia. As a result of this disease, other disorders in the structure of the valve apparatus may develop, for example:
- lengthening or shortening of the cardiac chords;
- improper attachment of the chords to the valve flaps;
- presence of additional chords;
As a result of structural changes in the connective tissue, degenerative processes occur in the valve leaflets, and they become more pliable. Because of this, the valve cannot withstand the pressure created by the left ventricle and bends towards the left atrium. Connective tissue dysplasia can occur for various reasons that affect the child in the womb, among them the following:
- Acute respiratory viral infections during pregnancy.
- The presence of occupational hazards in a woman.
- Preeclampsia.
- The influence of environmental factors on the mother during pregnancy.
- Excessive stress on the body of a pregnant woman.
In approximately 20% of cases, congenital MVP is transmitted through the maternal line. In addition, mitral valve prolapse occurs in other hereditary diseases, such as:
- Morphan's syndrome.
- Arachnodactyly.
- Elastic pseudoxanthoma.
- Osteogenesis imperfecta.
- Ehlers-Danlos syndrome.
Secondary MVP (or acquired) can occur as a result of certain diseases. The most common causes of this pathological condition are:
- Cardiac ischemia.
- Rheumatism.
- Hyperthyroidism.
- Chest injuries.
- Hypertrophic cardiomyopathy.
- Systemic lupus erythematosus.
- Myocardial dystrophy.
- Myocarditis.
Prolapse in this case occurs due to damage to the valve leaflets, papillary muscles, chordae or disturbances in the function and structure of the myocardium. Also, an important role in the mechanism of development of MVP is played by disturbances in the functioning of the autonomic nervous system, deficiency of micro- and macroelements (especially Magnesium) and metabolic pathology.
Another cause of secondary prolapse is aortic valve stenosis. As a result of this acquired defect, the opening of the aortic valve narrows, and blood cannot fully pass through it. This creates excess pressure in the left ventricle, which in turn presses on the bicuspid valve. If there is a fact of prolonged existence of excess pressure, then the mitral valve leaflets begin to bend towards the left atrium, and prolapse occurs.
Physical activity and sports
Is it possible to play sports with MVP?
Is it possible to play sports with prolapse? Mitral valve prolapse and sports - such a combination is very common among modern youth.
MVP is not a contraindication to sports or physical education, but the limitation directly depends on the degree of compensation. Thus, grade 1 prolapse does not limit the athlete’s physical activity; he can engage in almost all sports. For prolapse of the second degree, treatment is indicated, since it is dangerous with the risk of sudden death when engaging in exhausting physical exercise.
When engaging in sports such as weightlifting, lifting weights, or long-distance running, there is a colossal load on the heart and because of this, the risk of developing arrhythmia (fibrillation, atrial and ventricular flutter) increases tenfold, so we can say with confidence that MVP is dangerous with the risk of sudden death and there is repeated confirmation of this.
There have been so many deaths of young athletes right on the sports field, while help was provided immediately, but in most cases they could not be cured. Therefore, the doctor cannot 100% forbid you to engage in this or that sport, but you must understand that your health depends only on yourself and no one else, no one will force you to treat this or that disease.
Take care of yourself and then a long life is guaranteed.
With mitral valve prolapse, there are no clear recommendations that determine whether this sport is allowed for the patient or not. But there are some that are dangerous and traumatic for the heart.
It is important to remember that with the third degree of prolapse, sports activities are strictly contraindicated. There are certain restrictions for the first two:
- Run. If the disease is in the first degree, then you can run. This can be resolved in the second case only when diagnostic studies have confirmed compensation of blood circulation.
- Swimming. There are no restrictions for regular swimming, but synchronized swimming should be avoided. This is due to the fact that if the patient remains under water for a long time, he may lose consciousness.
- Workouts in the gym. If you have prolapse, you should not do any heavy lifting exercises. You should also avoid jumping. It is advisable to give preference to cardio exercises.
- Dancing. During a dance, a person moves in a fast rhythm. If the first degree of prolapse is diagnosed, then these hobbies do not need to be abandoned. But preference is advised to be given to types in which the partner is not supported, as this can cause disruption of blood flow in the brain and heart.
- Boxing. During such sports, a sudden blow to the chest may occur, causing the flaps to come off. Therefore, boxing is prohibited even in cases where prolapse is of the first degree.
The type of load is selected individually. Before training, you should discuss all the nuances with your doctor.
Symptoms of mitral valve prolapse
The severity of symptoms of mitral valve prolapse varies from minimal to significant and is determined by the degree of connective tissue dysplasia, the presence of regurgitation, and autonomic abnormalities. Some patients do not have any complaints, and mitral valve prolapse is an incidental finding on echocardiography.
In children with primary mitral valve prolapse, umbilical and inguinal hernias, hip dysplasia, joint hypermobility, scoliosis, flat feet, chest deformity, myopia, strabismus, nephroptosis, varicocele are often detected, indicating a disorder in the development of connective tissue structures. Many children are predisposed to frequent colds, sore throats, and exacerbations of chronic tonsillitis.
Quite often, mitral valve prolapse is accompanied by symptoms of neurocirculatory dystonia: cardialgia, tachycardia and interruptions in heart function, dizziness and fainting, vegetative crises, excessive sweating, nausea, a feeling of a “lump in the throat” and lack of air, migraine-like headaches. With significant hemodynamic disturbances, shortness of breath and increased fatigue occur. The course of mitral valve prolapse is characterized by affective disorders: depressive states, senestopathies, asthenic symptom complex (asthenia).
Clinical manifestations of secondary mitral valve prolapse are combined with symptoms of the underlying disease (rheumatic carditis, congenital heart defects, Marfan syndrome, etc.). Possible complications of mitral valve prolapse include life-threatening arrhythmias, infective endocarditis, thromboembolic syndrome (including stroke, pulmonary embolism), and sudden death.
Prolapse in childhood
In childhood, MV prolapse occurs much more often than in adults. This is evidenced by statistical data based on the results of ongoing research. It is noted that in adolescence, MVP is diagnosed twice as often in girls. Children's complaints are of the same type. Basically, this is an acute lack of air, heaviness in the heart and chest pain.
The most common diagnosis is grade 1 anterior leaflet prolapse. It was detected in 86% of examined children. Stage 2 disease occurs in only 11.5%. MVP III and IV with degree regurgitation are very rare, occurring in no more than 1 child out of 100.
Symptoms of MVP manifest themselves differently in children. Some people practically do not feel abnormal heart function. In others it manifests itself quite strongly.
- Thus, chest pain is experienced by almost 30% of adolescent children who have been diagnosed with MVC (mitral valve prolapse). It is caused by various reasons, among which the most common are the following:
- chords that are too tight;
- emotional stress or physical stress leading to tachycardia;
- oxygen starvation.
- The same number of children experience heart palpitations.
- Often teenagers who spend a lot of time at the computer, preferring mental activity to physical activity, are prone to fatigue. They often experience shortness of breath during physical education classes or when doing physical work.
- Children diagnosed with MVP often exhibit neuropsychological symptoms. They are prone to frequent mood swings, aggressiveness, and nervous breakdowns. Under emotional stress, they may experience short-term fainting.
During the examination of the patient, the cardiologist uses various diagnostic tests, through which the most accurate picture of MVP is revealed. The diagnosis is established when noises are detected during auscultation: holosystolic, isolated late systolic or in combination with clicks, isolated clicks (clicks).
Heart valve prolapse in childhood often develops due to a lack of magnesium ions. Magnesium deficiency disrupts the process of collagen production by fibroblasts. Along with a decrease in magnesium content in the blood and tissues, there is an increase in beta-endorphin and an imbalance in electrolyte balance. It has been noted that children diagnosed with MVP are underweight (inappropriate for height). Many of them have myopathy, flat feet, scoliosis, poor development of muscle tissue, and poor appetite.
It is recommended to treat MVP with a high degree of regurgitation in children and adolescents, taking into account their age group, gender and heredity. Based on the severity of the clinical manifestations of the disease, a treatment method is selected and medications are prescribed.
But the main emphasis is on changing the child’s living conditions. Their mental load needs to be adjusted. It must alternate with physical exercise. Children should visit a physical therapy room, where a qualified specialist will select the optimal set of exercises, taking into account the individual characteristics of the course of the disease. Swimming lessons are recommended.
With metabolic changes in the heart muscle
Symptoms of pathology
In most people, even proven mitral valve prolapse does not manifest itself in any way. The patients have no health complaints, the examination does not reveal clinically significant abnormalities. In this case, the detection of prolapse and mitral regurgitation of no higher than grade 1 on EchoCG in the absence of phenotypic signs indicates an asymptomatic variant or phenomenon of MVP.
If even minimal echocardiographic criteria for prolapse are accompanied by any symptom complexes characteristic of connective tissue dysplasia, then this is already a low-symptomatic option.
The first degree of mitral regurgitation does not lead to hemodynamic disturbances. Clinical manifestations begin from the second stage; it develops when myxomatous proliferation of the valve blades occurs (thickening of 3 mm or more), which in almost 100% of cases is caused by cardiovascular complications.
Symptoms of mitral valve prolapse are caused by its dysfunction. The most frequently recorded:
- feeling of interruptions and increased heartbeats;
- unrelated pain in the projection of the heart, resistant to nitroglycerin;
- atrioventricular blockade and various arrhythmias (ventricular extrasystole,);
- low load tolerance;
- dyspnea;
- clouding of consciousness, fainting;
- systolic murmur and systolic click (click).
Typically, the phenomena of valvular dysfunction are combined with autonomic disorders and other manifestations of connective tissue dysplasia. Their combined destructive effect reflects a clinically significant variant of the pathology.
The progression of mitral valve damage is the cause of dilatation of the left atrium and ventricle, the development of atrial fibrillation, atrial fibrillation, increasing heart failure, thromboembolism, chordal rupture and even sudden cardiac death. All this is a reflection of a morphologically significant variant of MVP.
The causes of the development of the defect are congenital and acquired.
Congenital causes
Anomalies in the development of connective tissue (Marfan and Ehlers-Danlos syndromes). This situation is genetically determined.
There are familial cases of pathology. In such families, all related members have this diagnosis confirmed.
| Causes of mitral valve prolapse | How common is it among all mitral valve pathologies? |
| Rheumatic mitral valve defects | 50–80% |
| For arterial hypertension and thickening of the myocardial wall of the left ventricle | 8–12% |
| Infectious endocarditis – damage to the valve apparatus by an infectious process (colonies of bacteria) | 10% |
| Severance of the chord as a consequence of blunt trauma to the chest and prolapse of the valve into the left atrium | No more than 2–3% |
| Prolapse and regurgitation due to avulsion of the leaflet chord during myocardial infarction | No more than 2–3% |
The most common cause of mitral prolapse is rheumatic defects. Rheumatism is an autoimmune pathology that leads to a change in the appearance of the valves and the development of prolapse and (or) stenosis - narrowing of the mitral valve opening.
In rheumatism, they speak of a combined mitral valve defect, in which regurgitation (backflow of blood into the atrium) can prevail over stenosis.
Why is mitral valve prolapse dangerous?
Are complications possible and what are the dangers of mitral valve prolapse? Despite the fact that in most cases there is mitral valve prolapse with minor regurgitation, which does not require special therapy, there is still a risk of complications. Complications are quite rare (only 2-4%) and include the following life-threatening conditions that require treatment in a specialized hospital:
- Acute mitral regurgitation is a condition that usually occurs as a result of separation of the chordae tendineae due to chest injuries. It is characterized by the formation of a “dangling” valve, that is, the valve is not held by the chords, and its valves are in free movement, not performing their functions. Clinically, a picture of pulmonary edema appears - severe shortness of breath at rest, especially in the lying position; forced sitting position (orthopnea), bubbling breathing; congestive wheezing in the lungs.
- Bacterial endocarditis is a disease in which microorganisms that have broken into the blood from a source of infection in the human body settle on the inner wall of the heart. Most often, endocarditis with damage to the heart valves develops after a sore throat in children, and the presence of initially altered valves can serve as an additional factor in the development of this disease. Two to three weeks after the infection, the patient develops repeated fever, chills, there may be a rash, an enlarged spleen, cyanosis (blue coloration of the skin). This is a serious disease that leads to the development of heart defects, gross deformation of the heart valves with dysfunction of the cardiovascular system. Prevention of bacterial endocarditis is timely sanitation of acute and chronic foci of infection (carious teeth, diseases of the ENT organs - adenoids, chronic inflammation of the tonsils), as well as prophylactic use of antibiotics during procedures such as tooth extraction, removal of tonsils.
- Sudden cardiac death is a serious complication, apparently characterized by the occurrence of idiopathic (sudden, causeless) ventricular fibrillation, which is a fatal arrhythmia.
Despite the fact that mitral valve prolapse rarely has a malignant course and causes severe complications, this disease still requires constant medical supervision and monitoring. Do not neglect your doctor’s recommendations and undergo regular check-ups with a cardiologist. Such measures will help you prevent the progression of this disease, and you will maintain your health and ability to work.
Diagnostics
Detection of MVP often occurs accidentally, and at any age, which, as already noted earlier, is accompanied by a cardiac ultrasound procedure. This method is the most effective in diagnosing mitral valve prolapse, because its use determines the possibility of identifying a specific degree of prolapse in combination with the amount of regurgitation accompanying the pathology.
- Mitral valve prolapse of the 1st degree determines the relevance for the patient of the variant of its manifestation in such a variant in which the bulging of the valves is insignificant (within 5 millimeters).
- Mitral valve prolapse of the 2nd degree determines the relevance of the bulging of the leaflets within no more than 9 millimeters.
- Mitral valve prolapse of the 3rd degree indicates protrusion of the leaflets of 10 millimeters or more.
It should be noted that in this version of dividing pathology into degrees, the degree of regurgitation is not taken into account, due to which now these degrees are not the basis for the subsequent determination of the prognosis for the patient and, accordingly, for the prescription of treatment. Thus, the degree of mitral valve insufficiency is determined on the basis of regurgitation, which is displayed to the greatest extent during ultrasound.
As additional diagnostic measures to determine the characteristics of the heart, an ECG procedure, as well as a Holter ECG, can be prescribed. Thanks to the ECG, it is possible to study changes relevant to the functioning of the heart based on the impact caused by mitral valve prolapse, while the Holter ECG allows recording of data relevant to the functioning of the heart within a period of 24 hours. Mostly, the congenital form of prolapse does not interfere with the functioning of the heart; accordingly, there is no special need for additional diagnostic measures due to the practical absence of detection of certain abnormalities in them.
Conservative treatment
As a rule, special treatment is not required for congenital prolapse. Treatment of the disease begins if:
- cardiopalmus,
- heart rhythm disturbance (arrhythmia),
- frequent autonomic disorders (chest pain, loss of consciousness, dizziness, etc.),
- severe mitral valve insufficiency.
The doctor selects the treatment method individually, depending on the symptoms, the degree of neglect of the disease and taking into account the characteristics of the patient’s body.
Mitral valve prolapse involves taking such groups of drugs as: beta blockers, antiplatelet and anticoagulant drugs.
Beta blockers slow down and reduce the force of heart contractions, which prevents abnormal heart rhythms. They also lower blood pressure and relax blood vessels, reducing their resistance to blood flow.
Antiplatelet drugs , based on aspirin, are prescribed both for prolapse and for stroke as a prophylaxis against thrombus formation.
Anticoagulant drugs are prescribed depending on the indications. They prevent blood clotting and also prevent the formation of blood clots. The most commonly used medicine in this group is warfarin. Treatment with anticoagulants is used for atrial fibrillation, heart failure, and also after a stroke. They must be taken strictly in accordance with the instructions of the attending physician; if they are violated, this can lead to dangerous complications.
If mitral valve prolapse is congenital, medications from the adrenergic blocking group (Propranolol, Atenolol, etc.) can be prescribed. They are indicated for use during attacks of tachycardia and as a prevention of arrhythmia. Magnesium-containing medications, for example Magnerot, are widely used. They improve the well-being of patients and fight the symptoms of vegetative-vascular dystonia. Treatment certainly includes taking vitamins, such as: riboflavin (vitamin B2), nicotinamide (vitamin PP) and Thiamine (vitamin B1).
Congenital mitral valve prolapse requires careful oral hygiene. It is recommended to brush your teeth twice a day, use dental floss, and visit your dentist twice a year. This will reduce the risk of developing such a serious complication of prolapse as infective endocarditis. You should also limit your consumption, or even better, completely abstain from alcohol, coffee, and cigarettes, as they contain substances that can impair the functioning of the heart.
The vast majority of people with prolapse are allowed physical daily household activities, but they should be moderate. Physical education for pathology without complications is encouraged. As for professional sports, this issue is resolved individually.
Treatment aims to prevent the progression of pathology.
This is largely facilitated by walking several kilometers and slow running with stops. Such exercises, combined with adherence to work and rest, the absence of emotional overload and overstrain from mental work, strengthen the heart.
However, patients with severe disease require long-term treatment with periodic monitoring of heart parameters, since in this case the pathology becomes dangerous, with unpredictable consequences. You may need to resort to surgery at any time.
How to treat mitral valve prolapse?
Treatment of acquired MVP in most cases is carried out in a cardiology hospital. The patient is recommended to adhere to bed or semi-bed rest, give up bad habits and follow a diet.
For rheumatic, i.e. infectious cause of the development of this heart defect, the patient is prescribed a course of antibacterial therapy to eliminate rheumatic carditis. For this purpose, antibiotics from the penicillin group are used (Billin, Vancomycin, etc.). If significant blood regurgitation and arrhythmia are detected in a patient, other medications may be prescribed, the action of which will be aimed at eliminating symptoms (diuretics, antiarrhythmics, hypotensives, etc.). The complex of therapy and dosage of drugs in such cases can only be selected individually. In the same way, the question of the possible need for surgical treatment is resolved.
To treat MVP, which was caused by cardiac pathologies, medications used to treat the underlying disease are used. This therapy is aimed at normalizing blood circulation and eliminating arterial hypertension and arrhythmias, and if drug treatment is ineffective, the patient may be recommended surgical intervention aimed at eliminating the mitral valve defect.
Particular attention is paid to cases of MVP that were caused by chest trauma. After correcting the condition with medication, patients undergo surgery to stabilize the mitral valve. Such patients require hospitalization and careful monitoring. If a cough with pink sputum appears, medical attention should be provided immediately, because any delay can lead to death.
Forecast for life
The prognosis for life is favorable. Complications rarely develop, and the patient’s quality of life does not suffer. However, the patient is contraindicated from engaging in certain sports (jumping, karate), as well as professions that overload the cardiovascular system (divers, pilots).
Regarding military service, we can say that, according to orders, suitability for military service is decided individually for each patient by a military medical commission. So, if a young man has mitral valve prolapse without regurgitation or with regurgitation of the 1st degree, then the patient is fit for service. If there is regurgitation of the 2nd degree, then the patient is conditionally fit (in peacetime he will not be called up). If there is grade 3 regurgitation, arrhythmias or heart failure of functional class 11 or higher, military service is contraindicated.
Thus, most often a patient with mitral valve prolapse with a favorable course and in the absence of complications can serve in the army.
Prolapse in pregnant women
Quite often, mitral valve prolapse is diagnosed in pregnant women during a complete mandatory examination. The first degree is usually not a concern. The pregnancy is proceeding normally, there are no negative consequences for the fetus. Moreover, prolapse can decrease during pregnancy: cardiac output increases, capillary resistance in the periphery decreases. Arrhythmias are possible, but childbirth occurs naturally and normally.
The addition of regurgitation or the transition of pathology to the second degree requires constant monitoring of the expectant mother by a cardiologist. Medicines are used only for health reasons (serious hemodynamic disturbances).
The rules of behavior for a pregnant woman with mitral valve prolapse are simple:
- avoid hypothermia and sudden temperature changes;
- move more to prevent congestion in the pelvic organs;
- rest in a reclining position.