A hypertensive crisis is a serious condition in which blood pressure levels critically increase. In this case, pronounced clinical symptoms are observed, and if they are not eliminated in a timely manner, severe complications that require other specific therapy. Prevention of a hypertensive crisis will help avoid negative consequences. What it is, more details in the article.
Pathogenesis of hypertensive crisis
The risk of developing a hypertensive crisis increases with:
- inadequate treatment of arterial hypertension (violations of the regimen or refusal to take medications);
- acute emotional distress;
- intense physical and psycho-emotional stress;
- acute alcohol intoxication.
Let us briefly point out that an acute increase in blood pressure during a hypertensive crisis (especially in the presence of initial vascular incompetence) may be accompanied by:
- disruption of autoregulation of organ (cerebral, coronary, placental, etc.) blood circulation;
- rupture of an atherosclerotic plaque with the formation of an intravascular thrombus and the development of acute ischemia;
- rupture of a microaneurysm (for cerebral blood flow) with the formation of hemorrhagic complications.
An overly aggressive decrease in blood pressure during the relief of a hypertensive crisis is an important risk factor for the development of various complications (the usual recommended rate of decrease in blood pressure is no faster than 20-25% of the initial one in the first few hours of treatment).
Causes
In addition to hypertension, a crisis can lead to other disorders, including the following:
- IHD (coronary heart disease);
- stroke;
- history of traumatic brain injury;
- kidney disease;
- hormonal and endocrine disorders;
- diabetes;
- atherosclerosis of the aorta;
- hyperthyroidism;
- pheochromocytoma;
- osteochondrosis;
- vegetative-vascular dystonia;
- prostate adenoma in men and menopause in women.
The causes of a hypertensive crisis may be of a different nature. For example, an attack can be provoked in the following cases:
- abusing caffeinated drinks, cigarettes and alcohol;
- not controlling the amount of salt in the diet;
- experiencing depression and stress;
- drinking excessive amounts of liquid;
- not observing sleep and rest patterns;
- experiencing intense physical exertion;
- consuming certain drugs without a doctor’s prescription, including potency enhancing drugs;
- independently prescribing and stopping antihypertensive drugs to stabilize blood pressure.
Abuse of caffeinated drinks, cigarettes and alcohol is a common cause of hypertensive crisis.
If each person can remove these factors from his life, then the reaction to changes in weather or climate zones does not depend on desire alone. Often, pressure surges are provoked by meteorological reasons.
Symptoms of hypertensive crisis
The most common symptom of a hypertensive crisis is encephalopathy, the development of which is associated with a violation of the autoregulation of cerebral blood flow, if the rapid rise in average pressure exceeds 110-180 mm Hg. In this case, brain hyperperfusion is observed. Under the influence of high intravascular pressure, fluid enters the extravasal space, and cerebral edema develops. Hypertensive encephalopathy manifests itself:
- headache,
- irritability,
- nausea,
- vomiting,
- dizziness,
- disturbance of consciousness.
Clinical examination of such patients reveals the presence of retinopathy (hemorrhages, exudates, swelling of the optic nerve nipple), local neurological symptoms. With target organ damage, signs of congestive heart failure, arrhythmia, proteinuria, moderate azotemia, and hypokalemia may occur.
The appearance of corresponding symptoms during a hypertensive crisis is associated with a violation of self-regulation of blood flow in vital organs (brain, heart, kidneys). In the case of a rapid increase in blood pressure, spasm of cerebral vessels occurs, and when blood pressure decreases, their expansion occurs. Normal cerebral blood flow remains constant when mean arterial pressure fluctuates between 60-150 mmHg. Art. In patients suffering from arterial hypertension (AH) for a long time, a decrease in cerebral blood flow is observed at a higher blood pressure than in healthy people, just as the lower limit of self-regulation in the case of a decrease in blood pressure is set at a higher level. In patients with arterial hypertension who receive adequate therapy, there is a tendency to normalize the self-regulation mechanism. The level of self-regulation is between the values inherent in healthy and untreated patients. At a lower level of self-regulation of cerebral blood flow in patients, blood pressure is on average 25% lower than average resting blood pressure.
The heart, unlike the brain, suffers less from a rapid decrease in blood pressure, since with a decrease in blood pressure, the myocardial oxygen demand is significantly reduced.
Diagnostics
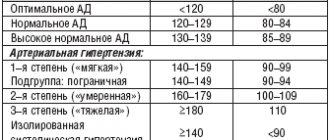
His treatment and recovery will depend on the correct and complete diagnosis of the patient’s condition. The first stage of diagnosis is to collect anamnesis. It is important for the doctor to find out how long the patient has been suffering from hypertension and whether there are concomitant diseases, whether crises are frequent and how long they last, what medications he takes on an ongoing basis. The main diagnostic indicator of a hypertensive crisis is blood pressure. Blood pressure during a hypertensive crisis will indicate its stage: in the first - 140/90, in the second - 160/100, in the third - 180/110 and higher. After the patient is hospitalized in the cardiology department, differential diagnosis is carried out to determine the presence of complications. The patient is prescribed:
- blood and urine tests;
- electrocardiogram;
- encephalogram;
- Holter blood pressure monitoring;
- Ultrasound of the kidneys;
- consultations of related specialists.
Return to contents
Complications of hypertensive crisis
Here is a list of complications during a hypertensive crisis:
- TIA (focal, cerebral and meningeal symptoms are eliminated in <24 hours); Currently, to establish this diagnosis, it is necessary to exclude asymptomatic cerebral infarction according to tomographic studies;
- acute hypertensive encephalopathy (general cerebral and meningeal symptoms are eliminated within <24 hours); the term “acute meningoencephalic edema” is sometimes used as a synonym;
- minor stroke (focal, cerebral and meningeal symptoms are eliminated in <3 weeks); the term “reversible neurological deficit” is also possible;
- cerebral infarction;
- hemorrhagic stroke : subarachnoid hemorrhages;
- parenchymal hemorrhages (hematomas, hemorrhagic impregnation);
- subarachnoid-parenchymal hemorrhages;
Causes and pathogenetic mechanism of development
The causes, duration and signs of a hypertensive crisis in women and men are somewhat different due to the physiological characteristics of the body and lifestyle. Psychosomatics explains this by differences in the lability of the nervous system. Among the common etiological provoking factors:
- hypertension;
- kidney diseases;
- endocrine and oncological diseases;
- nephropathology;
- nephropathy during pregnancy;
- weather sensitivity;
- regular stress;
- sudden withdrawal of antihypertensive drugs.
Types of hypertensive crises
Hypertensive crisis is divided into 2 types, which is determined by the severity of the course, the presence of complications and, accordingly, affects the management and treatment of the patient. It is impossible to make such a division based on the degree of increase in blood pressure.
Type 1 hypertensive crisis is characterized by a sharp increase in blood pressure without the appearance of new serious target organ damage.
Type 2 hypertensive crisis is different in that patients experience serious organ dysfunction even with relatively low blood pressure.
Hypertensive crisis type 1
With type 1 hypertensive crisis, blood pressure reaches 240/140 mm Hg. Art., there may be exudate in the retina and swelling of the optic nerve nipple. The lack of adequate therapy in many patients leads to rapid progression of the disease, and the course of arterial hypertension can become malignant. This type of crisis is recorded in patients with increased release of catecholamines (with pheochromocytoma, improper treatment with clonidine, use of sympathomimetics, cocaine). The main goal of treatment for such patients is to reduce blood pressure within 12-24 hours to a level of 160-170/100-110 mmHg. Art.
Hypertensive crisis type 2
Hypertensive crisis type 2 can be accompanied by relatively low blood pressure (160/110 mm Hg), but severe complications are detected:
- hypertensive encephalopathy,
- pulmonary edema,
- eclampsia,
- aortic dissection,
- cerebral hemorrhage or subarachnoid hemorrhage,
- unstable angina,
- myocardial infarction.
In such cases, it is necessary to ensure a decrease in blood pressure within 15 minutes to several hours.
Prevention and prognosis
The main place in preventing the development of hypertension and hypertensive crisis is given to normalizing the patient’s lifestyle and nutrition. Continuous use of antihypertensive medications, quitting smoking and alcohol, and avoiding stressful situations are important aspects of prevention. It is necessary to measure your blood pressure yourself daily and undergo a regular medical examination by a cardiologist. As for nutrition, it is recommended to avoid table salt, fried, smoked, pickled foods, spices, and caffeine-containing drinks. Prevention of a hypertensive crisis, strict implementation of all doctor’s recommendations and normalization of lifestyle make the prognosis of the condition positive.
Treatment of hypertensive crisis: first and emergency aid
In case of hypertensive crisis type 1, outpatient observation and treatment of the patient is possible.
A type 2 hypertensive crisis requires, after first aid, mandatory hospitalization and intensive monitoring of the patient’s condition. At the first examination of the patient, in addition to assessing complaints, previous history, the nature of the therapy, a physical examination is carried out to assess the condition of the central nervous system, heart, lungs, abdominal organs, pulsation of peripheral arteries. It is highly desirable to examine the fundus and urgently register an ECG. After this, antihypertensive therapy is selected and its initiation is ensured. Then, on an outpatient basis or in a hospital setting, laboratory tests are performed (biochemical parameters, general blood test, urine test) or other special studies to clarify the nature of the lesion in connection with the developed complication (ultrasound, X-ray, etc.).
In type 1 hypertensive crisis, preference is given to oral administration of drugs; in type 2 hypertensive crisis, preference is given to the parenteral route of administration.
For oral or sublingual administration today, captopril, nifedipine (Corinfar), clonidine (clonidine, gemiton) can be recommended, and for cardiac asthma - a combination of nitroglycerin with nifedipine.
Emergency care for hypertensive crisis
Nifedipine
Until recently, most recommendations for emergency care for hypertensive crisis included nifedipine as the drug of first choice. Preference was given to a capsule containing 10 mg of the drug, which is cracked and the contents are partially absorbed in the oral cavity and partially enter the stomach with saliva. After 15 minutes, if the pressure remains high, a second dose is recommended. The maximum effect after the first dose is achieved after 30 minutes. Therefore, if it is possible to wait this time, a repeat dose may not be necessary. Blood pressure usually decreases by about 25% after 10-15 minutes. Its excessive decrease is rarely recorded. Nifedipine increases cardiac output, coronary and cerebral blood flow and may increase heart rate, which should be taken into account when choosing it. But due to the emerging debate about the benefits and safety of short-acting calcium antagonists, the use of nifedipine has become limited in some countries.
The use of nifedipine is contraindicated in cases of unstable angina, myocardial infarction, and stroke.
Clonidine
In patients with clonidine withdrawal syndrome or in case of its improper use (monotherapy, rare doses of the drug and the presence of a long period between regular doses, etc.), preference is given to taking it sublingually in a dose of 0.125-0.2 mg. The drug reduces cardiac output and reduces cerebral blood flow. Therefore, in patients with heart failure, atherosclerosis of the cerebral arteries with encephalopathy, preference should be given to other drugs.
Captopril
In recent years, many publications have appeared on the use of captopril sublingually to reduce blood pressure during a hypertensive crisis. After taking 25 mg, within 10 minutes there is a decrease in blood pressure, which gradually increases and reaches its lowest value within 2 hours. On average, blood pressure decreases by 15-20% of the original level. After taking captopril, orthostatic hypotension may occur, and therefore the patient should remain in a horizontal position for several hours. In addition, one should remember the dangers of using captopril in patients with severe stenosis of the carotid arteries and aortic ostium.
The oral route of administration is more convenient, but intravenous infusion of short-acting drugs or repeated fractional intravenous administration of longer-acting drugs increases the safety of therapy and allows for a more rapid reduction in blood pressure.
In patients with a hypertensive crisis combined with a high content of catecholamines in the blood plasma (with pheochromocytoma, consumption of large amounts of foods rich in tyramine, especially when treating the patient with monoamine kinase inhibitors, clonidine withdrawal syndrome, taking or injecting sympathomimetics, cocaine), the drugs of choice may be prazosin, doxazosin, phentolamine (Regitin). In patients with clonidine withdrawal syndrome, the best effect is achieved by resuming its use.
Phentolamine is the first choice drug for pheochromocytoma and is administered intravenously at a dose of 2-5 mg. Prazosin can also be used, the first dose is 1 mg orally. After taking prazosin, the effect occurs within 0.5 hours. In this case, acute hypotension in orthostasis may occur (the effect of the first dose), to avoid which the patient should be in a horizontal position for 2-3 hours. A hypertensive crisis provoked by sympathomimetics or cocaine is treated with obzidan or labetalol. Labetalol (Trandate) can be given orally at a dose of 200 mg.
If complications occur during a hypertensive crisis, immediate initiation of controlled antihypertensive therapy through intravenous administration of antihypertensive drugs is necessary.
Treatment of hypertensive crisis during myocardial infarction
In patients with acute myocardial infarction, unstable angina, in order to reduce blood pressure and improve blood supply to the myocardium in the ischemic zone in the early stages against the background of pain, preference is given to infusions of nitroglycerin, nitrosorbide, and in the event of reflex tachycardia - in combination with β-blockers. The rate of administration is selected individually, starting at 5 mcg/min and increasing every 5-10 minutes until the systolic blood pressure drops to approximately 140 mmHg. Art. or the maximum nitroglycerin dose of 200 mcg/min is not achieved. Nitrosorbide (isoket) can also be used for this purpose. The initial rate of administration is 15 mcg/min and is gradually increased until the required hypotensive effect is achieved.
Treatment of hypertensive crisis in heart failure
In patients with heart failure that occurs in the first hours after the onset of myocardial infarction against the background of high blood pressure, the use of nitroglycerin or nitrosorbide should be preferred. In cases where pulmonary edema prevails and there is high pressure in the pulmonary artery, the administration of sodium nitroprusside is more effective.
In general, sodium nitroprusside is the most effective drug for patients in whom a hypertensive crisis is complicated by:
- severe pulmonary edema,
- dissecting aortic aneurysm,
- hypertensive encephalopathy.
Treatment of hypertensive crisis with pulmonary edema
In patients with hypertensive crisis and pulmonary edema, therapy includes the use of the following drugs:
- nitroglycerin,
- furosemide,
- morphine
- sodium nitroprusside.
Nitroglycerine
Taking nitroglycerin sublingually at a slightly higher dose (0.2-0.4 mg sublingually every 5 minutes) may be the first step in any setting. The drug at this dose dilates not only the veins, but also the arterioles, and therefore reduces the preload and afterload on the heart.
Furosemide
The loop diuretic furosemide is recommended to be used only in cases where hypovolemia is excluded, which is often detected during a hypertensive crisis with other complications. The dose of furosemide administered intravenously is 0.5-1 mg/kg. The diuretic effect manifests itself quickly, which suggests the need to provide appropriate conditions for the patient.
Morphine
It is better to administer morphine in fractional doses of 0.2-0.5 ml or 2-5 mg every 5-10 minutes if the attack does not stop.
What to do to prevent an attack from happening?
To prevent attacks, you need to know how to avoid a hypertensive crisis. The basic rules for preventing a hypertensive crisis are proper nutrition and a healthy lifestyle.
Active physical activity, walks in the fresh air and a good mood are the main factors that will help avoid attacks of high blood pressure..
You need to constantly monitor your blood pressure and if there are deviations from normal values, you should immediately consult a doctor. Failure to comply with the rules of prevention leads to increased blood pressure, and subsequently to a hypertensive crisis.
If you experience hypertension, you should consult a doctor. He will prescribe medication and indicate the individual dosage of medications that lower blood pressure.
In order to avoid a crisis, you need to take preventive measures . Recommendations for hypertensive crisis:
- give up any type of alcohol or reduce consumption to a minimum; for hypertension, alcohol is contraindicated;
- follow a diet: do not eat fatty and fried foods, limit spicy foods;
- bring body weight back to normal; overweight people are more prone to hypertensive crisis;
- eat no more than 7 g of salt;
- quit smoking;
- avoid nervous experiences.
If a person is often bothered by high blood pressure, he should spend more time outdoors and engage in active sports. This tones the body, normalizes all processes and restores health.
It is necessary to avoid overstraining the body and not to get carried away with heavy physical and cardio exercises, which affect the functioning of the heart and can lead to complications. When performing physical exercise, a hypertensive patient should closely monitor changes in pressure and not allow the readings to increase to 130 beats per minute.
The state of a person’s health, in particular blood pressure, largely depends on the person’s well-being, mood and attitude towards life. National recommendations for a hypertensive crisis: you should not focus on trifles and be sullen and aggressive.
A positive attitude towards the world and yourself will definitely result in a healthy and strong body for many years . A person should always be in harmony with nature and with life. If he loves life, then it will always reciprocate.
What types of vascular diseases exist? Preventive measures.
What drugs can be taken to treat hypertensive crisis? Read in this article.
Find out from this article whether a crisis can be treated with folk remedies.