What is Shereshevsky-Turner syndrome?
Shereshevsky-Turner syndrome (also called Shereshevsky syndrome, Turner syndrome) is a rare chromosomal disorder that affects women. The disorder is characterized by partial or complete loss (monosomy) of one of the second sex chromosomes. Turner syndrome is a highly variable condition and can present differently in each woman.
Affected women can potentially develop a wide variety of symptoms, affecting many different organ systems. Common symptoms include short stature and premature ovarian failure, which can lead to failure to reach puberty. Most women with Turner syndrome are infertile. A variety of additional symptoms may occur, including eye and ear abnormalities, skeletal malformations, and heart and kidney disease. Intelligence is usually normal, but affected people may have some learning disabilities.
Shereshevsky-Turner syndrome may be diagnosed before birth or shortly after birth or in early childhood. However, in some cases the disorder may not be diagnosed until adulthood, often by chance. In most cases, this disease does not run in families and occurs randomly for no apparent reason (sporadic).
Shereshevsky-Turner syndrome is one of the most common chromosomal disorders and probably the most common genetic disorder in women.
Risks of anomaly
The likelihood of having a child with Shereshevsky-Turner syndrome is not related to the age of the mother. The anomaly in one form or another occurs in 1% of all conceptions, and most embryos die before birth as a result of miscarriage or frozen pregnancy. In 10% of miscarriages, the cause is monosomy X in the fetus.
Only 1% of such pregnancies last until the 7th month. If a child is born viable, he can live a normal life. Most of these girls are diagnosed with infertility, although with the mosaic form the likelihood of becoming pregnant is higher than with the true form.
Symptoms and signs
The symptoms and severity of Shereshevsky syndrome can vary from one person to another. Many signs of the disorder are nonspecific, and others may develop slowly or may not be noticeable. It is important to note that affected people may not have all of the symptoms described below. Affected families should talk with doctors about their specific case, associated symptoms, and overall prognosis.
Skin fold on the neck.
The anomaly is considered one of the most common manifestations of the syndrome (in 70% of cases). It looks like a wing-shaped seal that runs from the back of the head to the trapezius muscles.
With a significant excess of skin, a visible membrane appears, stretched between the head and shoulders. Such a cosmetic defect can be corrected with a simple operation.
Small growth.
In newborns with a genetic disorder, body length varies between 42-45 cm. However, with the mosaic form of the syndrome, growth may be normal. Development occurs with a lag according to the female type.
Sometimes short stature is caused by a disorder in the formation of the spinal column (vertebral fusion or deformity).
"The Face of the Sphinx"
The symptom can also occur in other diseases, but in Shereshevsky-Turner syndrome it is diagnosed in 35% of cases and is supplemented by cervical skin pathology.
The person has thickened lips (see photo), and there are no natural folds in the forehead area (“polished forehead”). It is difficult for him to close his eyelids completely. Facial expressions are usually difficult (due to congenital weakness of the facial muscles).
Barrel-shaped or flattened chest.
In the first case, the frontal and anteroposterior dimensions of the chest are almost the same. Deformation occurs in 45% of cases of anomaly.
If there is a defect in the formation of the bones of the chest, its flattening is noted.
With moderately severe pathologies of the development of the skeletal system, the sign may become less noticeable with age. The violation cannot be corrected surgically. Usually such influence is not necessary. The defect does not cause changes in the functioning of the heart or respiratory system.
Swelling.
Edema is usually localized in the area of the feet or legs and is considered a specific symptom (occurs with varying degrees of severity in more than 50% of patients). Nails look squeezed. In the presence of congenital malformations, swelling can be very severe.
Poor weight gain.
The weight of newborn babies with Turner syndrome ranges from 2500–2800 g, falling within the normal range. But as the baby grows, body weight gain deviates from optimal values. In the future, he will always be worse than his peers.
Improper development of the ears.
The ears are usually located below eye level. The cartilage that forms the ears in people with Shereshevsky syndrome is often underdeveloped and can cause hearing loss.
Epicanthus.
This is the name for the formation of a skin fold in the inner corner of the eye (see photo). In this case, there is no combination with a Mongoloid incision (as in children with Down syndrome).
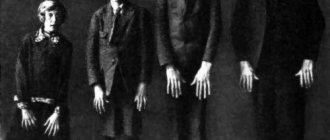
Valgus curvature of the elbows.
Pathological curvature of the elbows, when the lowered arm is unable to straighten and deviates to the side of the body. It is observed in almost 65% of patients with the disease. A similar anomaly can be diagnosed in the knee joints, making walking difficult.
Finger deformities.
Finger deformities (little finger clinodactyly, syndactyly) are diagnosed in 75% of cases. They are not always noticeable in infants, and often become apparent as they grow older.
Abnormal position of the nipples.
An increased distance between the nipples on the chest is a typical sign of an anomaly only when combined with other manifestations of Turner syndrome. It is observed in 35% of patients with chromosomal pathology.
Skin hyperpigmentation.
The sign is observed in 35% of cases of Shereshevsky-Turner pathology and is not considered specific. The accumulation of pigment can provoke endocrine disorders. Pathological formations manifest themselves in the form of nevi and birthmarks.
Cardiovascular pathologies.
The most common cardiovascular problems in Shereshevsky-Turner syndrome are patent ductus arteriosus, ventricular septal defect, coarctation or aortic aneurysm.
Heart defects associated with some cases of Turner syndrome may increase the risk of severe, life-threatening complications, including high blood pressure in the arteries of the lungs (pulmonary hypertension) or aortic dissection, a condition in which there is a tear in the inner wall of the aorta. Blood rushes into the middle layer of the aorta, causing the middle and inner layers to separate (dissect). Aortic dissection can cause the outer wall of the aorta to rupture.
In some cases, kidney disease may occur, including horseshoe kidneys or absent (agenesis) kidneys. Kidney abnormalities increase the risk of urinary tract infections and high blood pressure (hypertension).
Intelligence in women with Turner syndrome is usually normal. However, affected women may develop learning difficulties, especially difficulties with visual-spatial relationships. An example would be right-to-left disorientation. Those affected may have difficulty learning math, nonverbal memory, and attention. Affected women may also experience difficulties in certain social situations.
Some people with Turner syndrome are at higher risk of developing certain disorders, including Hashimoto's thyroiditis, inflammatory bowel disease, hypothyroidism, vitiligo, osteoporosis, hair loss, hypertrichosis, diabetes, celiac disease, obesity, and coronary heart disease. The risk of colon cancer is greatly increased.
Causes
Shereshevsky-Turner syndrome is caused by partial or complete loss (monosomy) of the second sex chromosome. Chromosomes are found in the nucleus of all cells in the body. They carry the genetic characteristics of each person and come in pairs. We receive one copy from each parent. Chromosomes are numbered 1 to 22; The 23rd pair usually consists of one X and one Y chromosome for males and two X chromosomes for females. Thus, women with a normal chromosomal structure (karyotype) have 46 chromosomes, including two X chromosomes (46, XX karyotype). Each chromosome has a short arm, designated "p", and a long arm, designated "q". The chromosomes are further divided into many numbered bands.
Women with Turner syndrome are missing all or part of the second sex chromosome. The reason why this occurs is unknown and is believed to be the result of a random event. In some cases, the chromosomal abnormality appears to occur spontaneously due to an error in the division of the parent's reproductive cells, either in the father's sperm or in the mother's egg. This leads to the fact that the genetic error appears in all cells of the body.
In many cases, only a certain percentage of a person's cells may be affected. This is called mosaicism. Specifically, some cells have the normal 46 chromosomes (one cell line), while other cells do not have the normal 46 chromosomes (the second cell line). This second cell line may contain various abnormalities, such as partial or complete loss of the X chromosome. In these cases, the loss of genetic material from the X chromosome usually occurs due to spontaneous errors very early during fetal development. Theoretically, in people with mosaicism, Turner syndrome may cause fewer developmental problems than in other cases because fewer cells are affected. However, this is difficult to predict.
In some cases, rarer chromosomal abnormalities (other than complete or partial monosomy) can cause the syndrome. Such abnormalities include a ring chromosome or isochromosome X. Ring chromosomes occur when the ends of a chromosome break off and the long and short arms join together to form a ring. Isochromosomes occur when one part of a chromosome is missing and replaced by an identical version of another branch.
In rare cases, some cells have one copy of the X chromosome, while other cells have one copy of the X chromosome and some Y chromosome material. The amount of Y chromosome material is not enough to cause the development of any male characteristics, but is associated with an increased risk of developing a form of cancer known as gonadoblastoma.
Most symptoms of Shereshevsky-Turner syndrome occur due to the loss of specific genetic material from one of the X chromosomes. So far, one gene, SHOX, is known to play a role in the development of the syndrome. The SHOX gene codes for a protein that helps regulate other genes in the body. The protein product of the SHOX gene plays a role in skeletal growth and maturation. Researchers believe that the loss of one SHOX gene on the altered X chromosome is the main cause of short stature in women with Turner syndrome.
Affected Populations
Shereshevsky syndrome affects approximately 1 woman in 2000-2500 live births. There are no known racial or ethnic factors that influence the incidence of the disorder. In some cases, the disorder is diagnosed before birth or shortly after birth. However, mild cases may remain undetected until later in life and even into adulthood.
Turner syndrome and society
The incidence of the syndrome is one case per 2-5 thousand newborn girls. Persons with monosomy of sex chromosomes require social adaptation in society. This is a complex problem that requires large financial and psycho-emotional costs. From early childhood, the child feels inferior due to developmental delays and short stature. Girls in puberty develop complexes about the underdevelopment of secondary sexual characteristics (lack of mammary glands, normal hair growth in typical places, female body type). For a long time they continue to remain children with an infantile perception of the world in adulthood. Naturally, all this leaves its negative imprint on the development of the individual. Therefore, it is important to inform the population about the presence of genetic pathology, so that each person can correctly perceive such patients, understanding their problem, and not considering inferiority. Teaching society such a culture will make the lives of sick people much easier.
Important to remember!!! Social rehabilitation is one of the most important elements of a full life for patients with chromosomal abnormalities.
Diagnostics
During pregnancy, the syndrome can be suspected during an ultrasound examination. With Shereshevsky-Turner syndrome, some physical abnormalities appear:
- thickening of the collar area;
- cervical hygroma;
- expansion of the renal pelvis and calyces;
- deformation of bones, shape of the head, limbs;
- heart defects;
- oligohydramnios or polyhydramnios.
Thickening of the nuchal translucency and hygroma are noticeable already at the first planned ultrasound. With the mosaic type of pathology, the results of ultrasound diagnostics remain normal.
To clarify the form of the disorder, fetal karyotyping is recommended. The study is carried out from 10 to 12 weeks of pregnancy.
When performing this procedure (under ultrasound control), a special needle (inserted into the uterine cavity through the anterior abdominal wall) or a catheter (through the cervix) is used to collect amniotic fluid (amniocentesis), blood from the umbilical cord vessels (cordocentesis) or a sample of fetal cells (biopsy). chorion).
Diagnostic measures
Identification of the syndrome during pregnancy is rare. During a routine ultrasound examination, it is almost impossible to examine the folds on the fetal neck. Perinatal research methods are performed according to strict indications, as they can be dangerous to the fetus. If the development of Shereshevsky-Turner syndrome is suspected, invasive diagnostic methods are used. Genetic tests, chorionic villus biopsy, cordocentesis, and amniocentesis are performed.
After the birth of a newborn, the primary diagnosis is established if characteristic external manifestations are detected during examination. Karyotyping helps confirm or refute the diagnosis. Geneticists study each chromosome and describe specific characteristics. The shape, structure, and parameters of the chromosomal structure are considered.
Additional studies are carried out to differentiate the pathology from some others with similar symptoms. Similar psychoneurological and physiological signs are observed in patients with Noonan and Rokitansky-Kustner-Mayer syndromes. Additional diagnostic methods:
- Ultrasound of internal organs;
- cardiogram to study the functioning of the heart;
- general blood test, urine test;
- determination of sex chromatin;
- hormone analysis;
- X-ray of the bones of the feet and hands;
- MRI, CT.
A geneticist conducts a survey of parents to identify factors that may influence the occurrence of the syndrome: alcoholism, exhaustion. It is being determined whether there were any genetic diseases in the family up to the fourth generation. In addition to a geneticist, examination by specialized specialists will be required.
Chromosomal pathology is diagnosed in children of healthy parents. It is impossible to foresee the possibility of the development of the syndrome, as well as to take any preventive measures.
The only way to detect X chromosome deficiency is to undergo prenatal diagnosis in the early stages of pregnancy. At 11–13 weeks, a woman can donate blood to check for the presence of plasma protein A. This means an increased likelihood of a genetic abnormality. The diagnosis can be confirmed or refuted using chorionic villus biopsy. They are used to determine the fetal karyotype and chromosome structure.
If the syndrome is detected at the gestation stage, there is no need to panic. A girl can be born without external manifestations of the disease, and the underdevelopment of the genital organs is corrected with the help of hormonal therapy.
Treatment
Treatment for Shereshevsky-Turner syndrome targets the specific symptoms that occur in each person. Treatment may require the coordinated efforts of a team of specialists. Pediatricians, pediatric specialists, surgeons, cardiologists, endocrinologists, speech therapists, otolaryngologists, ophthalmologists, psychologists, and other health care providers may need to plan systematically and comprehensively for a child's affective treatment. Genetic counseling is recommended for affected individuals and their families.
Specific therapeutic procedures and interventions may vary depending on a variety of factors, such as the severity of the disease; the presence or absence of certain symptoms; the person's age and general health. Decisions regarding the use of specific drug regimens and/or other treatments should be made by physicians and other members of the health care team in careful consultation with the patient based on the circumstances of the case; careful discussion of potential benefits and risks, including possible side effects and long-term consequences; patient preferences; and other relevant factors.
There is no cure for Shereshevsky syndrome, but treatments have been developed that can improve physical development. With proper medical care, women with Turner syndrome should be able to lead full, productive lives. The main methods of treating sick people are therapy with growth hormones and estrogens.
Individuals with Turner syndrome may benefit from growth hormone (GH) therapy, which can help normalize height. The Food and Drug Administration (FDA) has approved the use of recombinant growth hormone to treat children with Turner syndrome. Recombinant GH is artificially created in the laboratory. The best age to initiate GH therapy and the optimal duration of therapy in women with the syndrome are unknown. Generally, the earlier GH therapy is started, the more beneficial it is for those affected. However, there are many individual factors that ultimately determine the effectiveness of growth hormone therapy. Decisions regarding GH therapy in individuals with Shereshevsky syndrome are best made in consultation with a pediatric endocrinologist.
Most women with Turner syndrome require sex hormone replacement therapy to undergo the normal development associated with puberty and begin menstruation. Replacement therapy using estrogen and progesterone typically promotes puberty and the development of secondary sexual characteristics. Replacement therapy with these hormones usually begins around the age of 12-14 years. It is at this time that most average girls enter puberty.
Most women with Turner syndrome remain unable to conceive children. In vitro fertilization (IVF) using a donor egg and an implanted pregnancy is sometimes possible. In most cases, these pregnancies are risky and require close consultation with your doctor.
Additional treatment is symptomatic and supportive. For example, hormone replacement therapy can be used to treat people with thyroid disease. Correcting hearing loss with hearing aids is another important intervention that can help with learning and social interaction.
Early intervention is important to ensure that children with the syndrome reach their potential. Special services that may be helpful for affected children may include special psychosocial support, speech therapy, and other similar services.
Forecast
The prognosis for Turner syndrome is favorable in terms of life expectancy and intellectual development. The exception is when:
- congenital heart defects;
- spina bifida;
- abnormal formation of the genitourinary system.
As for the restoration of reproductive function, most patients remain infertile. However, with adequate and timely therapy, women can create families, lead a full sex life, and give birth to children.
Shereshevsky-Turner syndrome is a complex genetic pathology that affects the entire body. However, with timely diagnosis and proper treatment, patients have a chance to adapt to society.