Medical Consultant Vessels and Heart Hemorrhagic vasculitis: signs, symptoms and treatment
This disease, medically called Henoch-Schönlein syndrome or allergic (rheumatic) purpura, is diagnosed mainly in patients aged 5-13 years. In adults, cases of hemorrhagic vasculitis are also common.
It occurs less frequently in children under 3 years of age. The development of this disease is always associated with damage to the walls of vascular beds, an increase in the degree of their permeability, activation of the protein metabolism process, and increased production of immune responses.
- Signs and symptoms of hemorrhagic vasculitis, photo
- Forms of hemorrhagic vasculitis
Hemorrhagic vasculitis: skin-articular form
- Complications of hemorrhagic vasculitis
Causes
Hemorrhagic vasculitis is a vascular diathesis caused by an allergic reaction to small vessels. Allergies can be caused by:
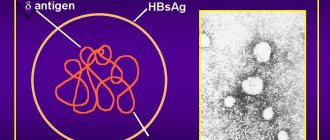
• microbes (60-70 percent of patients have a history of upper respiratory tract infections, most often caused by streptococci. Other microorganisms that can contribute to the development of the disease are rubella, chicken pox, measles, HIV);
• some medications;
• vaccines;
• insect bites;
• exposure to cold;
• various chemicals;
• food allergens (nuts, eggs, meat, milk, tomatoes, fish, chocolate).
As a result of an allergic reaction, the body begins to produce IgA antibodies, which accumulate in excess in the blood vessels of the skin, as well as in the joints, digestive tract, kidneys, central nervous system or testicles. As a result, inflammation develops in these places.
Hemorrhagic vasculitis: what is it?
Hemorrhagic vasculitis is a systemic disease of a series of vasculitis, characterized by damage to the walls of the smallest vessels of the body - capillaries, venules and arterioles. This condition is always accompanied by a violation of the structure of these blood vessels.
As a rule, the disease occurs with the presence of aseptic inflammation, which significantly increases the likelihood of blood clots. In the presence of rheumatic purpura, not only the blood vessels of the skin are affected, but also the internal organs (joints, kidneys, gastrointestinal tract).
Causes of hemorrhagic vasculitis
The main trigger of this disease is infection of various etiologies. These could be fungi, bacteria or viruses. The development of the disease is also influenced by the use of certain medications and the unfavorable environmental conditions in which the patient lives.
Predisposing factors to the occurrence of hemorrhagic vasculitis are:
- insect bites;
- thermal burns;
- injuries of various origins;
- intoxication due to biological poisons entering the body;
- vaccination procedures;
- congenital functional disorders of the immune system;
- colds;
- overheating or hypothermia of the body;
- allergic reactions caused by food agents.
The danger of sunburn for the human body, their treatment and prevention of complications:
Pathomorphology
The pathomorphology (pathological anatomy) of hemorrhagic vasculitis consists of abnormally increased capillary permeability (capillary toxicosis). Initially, due to the expansion of capillaries, extravasation of blood plasma occurs, and subsequently diapedesis of erythrocytes into the surrounding tissues; As a result, rashes develop, which subsequently become hemorrhagic in nature. The described sequence of events (first transudation, then hemorrhage) is not mandatory. Often, hemorrhages may appear on the skin without preliminary swelling (as well as with capillary toxicoses of infectious origin - typhus, sepsis, hemorrhagic measles, smallpox, etc.).
Vasomotor phenomena are usually accompanied by inflammatory phenomena; Thus, spastic colic and intestinal bleeding develop into mucohemorrhagic colitis, hematuria into nephritis, which is usually acute, but sometimes takes a chronic course. In other cases, the process follows the path of necrobiosis with the development of necrotic areas.
Causes
The disease occurs as a result of immune disorders in the body. The causes of vasculitis are:
- acute, chronic infections of a bacterial or viral nature;
- hereditary predisposition;
- individual reaction of the body to vaccination;
- poisoning with biological poisons, chemicals included in certain drugs (for the treatment of oncology);
- severe overheating of the body or, conversely, hypothermia;
- injuries of various origins and localization;
- thermal damage to the skin (sunburn).
Symptoms and clinical picture
There are four clinical forms of hemorrhagic vasculitis:
• simple;
• rheumatoid;
• abdominal;
• lightning fast.
The first two forms were described by Schönlein, the last two by Henoch. These forms are found in all possible combinations and mutually transform into one another.
This disease is not so much hemorrhagic as a transudative-exudative diathesis of a facultative hemorrhagic nature. Isolated, sharply demarcated rashes on the skin (as well as on the mucous membranes) are initially erythematous, papular or urticarial in nature, often painful and accompanied by itching; subsequently, within a few hours, these rashes become hemorrhagic. Since not all elements develop simultaneously, rashes are observed on the skin in various stages of development - from hyperemia and subcutaneous edema to persistent erythema, from serous impregnation to hemorrhages of varying duration and different colors (blue-purple, brown-black, pale yellow and etc.). The result is a motley picture, very reminiscent of erythema multiforme exudative. Skin infiltrates, as with erythema nodosum, and an itchy urticarial rash, and angioedema (on the face, genitals, etc.) are also observed.
The described changes in the skin may be the only symptom of hemorrhagic vasculitis or, as is more often the case, they accompany manifestations of the same diathesis in the joints or internal organs. Mild forms, expressed by skin rashes, general weakness and a slight increase in temperature, are designated as simple purpura. This disease usually lasts no more than 2 weeks, but sometimes relapses are observed, in particular due to the patient getting up early (orthostatic purpura).
Rheumatoid purpura is close to this form, differing from simple purpura by damage to the joints, most often the knees, in which hemorrhages occur with a slight exudation of serous exudate, which causes swelling and aching in the joints. These phenomena resemble, on the one hand, rheumatic pain (hence the name “rheumatoid purpura”), and on the other, arthralgia during serum sickness.
With the addition of the above-described picture of damage to internal organs, a symptom complex of abdominal purpura arises. In its most typical form, it occurs mainly in childhood and adolescence. Usually, all symptoms are pronounced at the end of or soon after an infectious disease (tonsillitis, measles, scarlet fever, typhoid fever), often as a complication of pulmonary tuberculosis. The disease occurs in paroxysms, in the form of intestinal colic, accompanied by bloody stools and vomiting mixed with blood. Its morphological substrate is transudative-hemorrhagic rashes on the mucous membrane of the stomach and intestines; Later, these rashes are complicated by exudative-inflammatory phenomena, as a result of which the initial functional disorders of the intestine (colospasm) acquire a more persistent, organic character (hemocolitis). Often, hemorrhages throughout the entire thickness of the intestinal wall are complicated by intussusception into the affected stretched and relaxed areas of the overlying parts of the intestines, which have retained their peristalsis.
The general picture of the disease - a swollen, tense and painful abdomen, a suffering appearance of the patient, a rapid and small pulse - is so reminiscent of the symptom complex of an acute abdomen that such patients are sometimes referred for laparotomy. The erroneous diagnosis of “acute abdomen” becomes obvious if you only pay attention to the accompanying phenomena of the skin and joints. In addition, abdominal purpura often occurs with symptoms of hemorrhagic nephritis, and sometimes hemorrhagic pleurisy. Women may experience uterine bleeding. The variety of combinations and the simultaneity of damage to many organs suggests that changes in the abdomen are not local in nature, but are a partial expression of a general transudative-hemorrhagic diathesis. As soon as bloody bowel movements, vomiting, and colic disappear, the patient gives the impression of being completely recovered. Such attacks can be repeated many times at intervals of several days, or even several weeks.
Hemorrhagic vasculitis, as a rule, occurs with an irregular temperature, sometimes up to 38-40°C. The genesis of fever is toxic-allergic. Thus, the symptomatology of the disease is very diverse depending on the location of the process.
In extremely rare cases, a picture of a true acute abdomen that requires surgical intervention may actually arise due to necrosis that occurs due to massive hemorrhages into the mucous membrane and submucosa, disrupting the nutrition of the intestinal wall.
Damage to the nostrils in hemorrhagic vasculitis usually occurs in the 2-3rd week from the onset of the disease, but in the chronically recurrent form it can only be detected in the final stage of the disease.
In the clinic of hemorrhagic vasculitis, all gradations of kidney damage are observed - from mild, asymptomatic, focal, to severe diffuse glomerulonephritis with symptoms of renal failure. In some cases, a picture of subacute malignant extracapillary nephritis develops with rapid evolution within 4-5 months from the onset of the disease to death from uremia.
An extremely severe course of the disease is characteristic of fulminant purpura. Like the abdominal form described above, fulminant purpura most often occurs in children in connection with past infectious diseases - severe forms of scarlet fever, tonsillitis, pneumonia. With this form of purpura, all the manifestations characteristic of the forms described above are observed, but to a more severe, “superior”, so to speak, degree. Skin rashes take on a confluent character, forming extensive hemorrhagic surfaces rising above the skin level; subsequently, necrotic changes occur in the center of these hemorrhagic areas, and rather deep ulcerative defects with an edematous shaft in the circumference are obtained.
Treatment of hemorrhagic vasculitis
Traditional methods
The duration and nature of treatment for hemorrhagic vasculitis in children and adults depend on the severity, clinical form and phase of its development. For all forms of the disease, antiplatelet agents - Trental and Curantil - are prescribed. In particularly severe cases, in order to enhance the antiaggregation effect, the patient is prescribed two of these drugs simultaneously.
Anticoagulants are also prescribed. The dose schedule, single and daily dosages are selected individually for each patient. Patients are often prescribed intravenous or subcutaneous administration of Heparin. In the second option, the medicine enters the body through fatty tissue in the abdominal cavity.
If necessary, the doctor prescribes fibrinolysis activators. These are nicotinic acid and all its derivatives. In addition to these drugs, the following are prescribed:
- glucocorticosteroids;
- vitamins E and A;
- membrane stabilizers;
- cytostatics;
- analgesics;
- antispasmodics;
- enterosorbents;
- anti-inflammatory.
When treating hemorrhagic vasculitis in adults, plasmapheresis may be indicated. The method of implementation is selected based on the severity of the pathology. Through plasmapheresis, it is possible to achieve purification of blood plasma from toxic agents at the molecular level.
Surgery
Surgical methods of treatment are carried out in extreme cases - when transplantation of a new kidney is required to replace the damaged one, the functions of which cannot be restored. Surgery can also be performed on the intestines to remove the affected area.
Hemorrhagic vasculitis in the ICD is classified as a severe vascular pathology and is one of the types of immune vasculitis. It is designated by code D69.0 and is more often called allergic purpura.
Traditional methods
1. Pass 3 lemons and 2 pcs. through a meat grinder. cloves (spice). Add 500 g of sugar to the mixture and fill with warm water (1.5 l). Place the mixture in a glass jar with a lid and store it in a dark place for 15 days. After the expiration date, take the product three times a day before meals, 15 g.
2. Grind 5 parts of rue leaves and add 1 part of butter to them (can be replaced with vegetable oil). Mix thoroughly and place in a glass container, which is left for 10 days in a dark, dry place. When the mixture is infused, rub it 4 times a day into the affected areas.
3. Finely chop and mix the herbs (10 g each): mint, marigold, horsetail, string, poplar buds, elderberry and yarrow. Every morning, pour 10 g of herbal mixture with boiling water (300 ml), leave, strain and drink the infusion, dividing it into three doses.
Course of the disease
The course of hemorrhagic vasculitis has a wide range - from an acute fulminant form lasting several days to a long-term, chronically recurrent form over a number of years. The chronically relapsing form is characterized by repeated acute attacks, each of which has its own characteristics: for example, if the first attack occurs in the form of rheumatoid purpura, with joint pain and skin rashes, then subsequent attacks can give a picture of acute abdomen, hemocolitis or hematuric nephritis. Following the attack, remission occurs.
Along with long-term, persistently recurrent forms, mild forms are known, ending in a short period of time with complete self-healing.
Vasculitis in adults: treatment
If the abdominal form is observed in adults, then intravenous nutrition is necessary. Doctors recommend taking medications that prevent vomiting, as well as drugs that can relieve the patient from pain.
If the patient notices bleeding during bowel movements, doctors recommend such remedies as Heparin and antiaggregants. Medicines are also used that are aimed at avoiding the occurrence of an allergic reaction. Immunosuppressants are used to activate the immune system. Prednisolone is mandatory .
As the disease progresses, patients are given plasma transfusions . Plasmapheresis is also recommended . A rash in adults must be treated in a hospital to prevent the pathology from becoming a chronic type of disease.
Diagnostics
The diagnosis of hemorrhagic vasculitis is based on the following features:
• presence of hemorrhagic skin rashes;
• diversity of the clinical picture: along with abdominal phenomena, either joint phenomena or bleeding from the gastrointestinal tract are observed;
• negative clinical and laboratory tests.
The study of hemorrhagic syndrome (both the blood coagulation system and the whole, and its individual components), the duration of bleeding, and clot retraction are normal. The number of blood platelets is also normal. Symptoms of a pinch or tourniquet are not constant.
Differential diagnosis is especially important in cases of abdominal purpura, simulating the picture of an acute abdomen (perforated peritonitis, acute appendicitis, intussusception).
In these cases, the diagnosis is often made on the operating table - after detection of hemorrhagic rashes on the peritoneum and serous intestine. The following signs serve as reference points in diagnosis:
• with a general picture of an acute abdomen, the abdomen is actually soft;
• abdominal pain is often cramping in nature, often localized around the navel (but can also be localized in the cecal region, simulating the picture of acute appendicitis);
• along with abdominal symptoms, either joint phenomena or bleeding are observed - from the gastrointestinal tract, kidneys, genitals, etc.;
• although leukocytosis can sometimes be very high (up to 30 thousand), the blood is not “purulent”: there is no toxogenic granularity of neutrophils, eosinophils do not disappear.
Diagnosis can be made by testing blood (detecting elevated levels of IgA) and urine (blood in the urine) or stool (occult blood test). If symptoms of severe renal failure occur, a biopsy of this organ is required.
Differences in symptoms between adults and children
Hemorrhagic vasculitis in adults and children is significantly different. In adults, the onset of the disease is very difficult to determine, because the symptoms are minor, intestinal problems are observed in less than 50% of patients, deterioration in kidney function, and rashes in a small area are possible.
With the onset of the disease, children develop a high fever, loose stools with drops of blood, and also kidney failure; the rash covers a large part of the skin.
Treatment
If the inflammation has not affected the organs, including the kidneys or gastrointestinal tract, only symptomatic treatment of hemorrhagic vasculitis is used. The patient may be prescribed hemostatic drugs (etamzilate), antihistamines and non-steroidal anti-inflammatory drugs (with the exception of aspirin, which can aggravate the symptoms of the disease), and glucocorticosteroids. Skin lesions heal well with dapsone.
If the kidneys are affected, immunosuppressive drugs are used to weaken the immune system, preventing further kidney damage.
Diagnosis of hemorrhagic vasculitis
The changes that the patient’s biological samples undergo during laboratory examination cannot be called specific. To confirm the diagnosis, pay attention to the level of:
- ESR;
- platelets;
- leukocytes;
- alpha-2-globulins;
- immunoglobulins A and G;
- reactive proteins;
- seromucoids;
- fibrinolysis;
- fibrinogen;
- cryoglobulins;
- DFA;
- antihyaluronidase;
- fibrin monomers;
- antistreptolysin.
During research, it is necessary to differentiate hemorrhagic vasculitis. Diagnosing the disease is not difficult for doctors.
The difficulty may lie only in determining its form of development and the possibility of confusing, for example, the abdominal form of pathology with some other disease:
- intestinal obstruction;
- pancreatitis;
- cholecystitis;
- peritonitis;
- inflammation of the appendix.
Also, hemorrhagic papules can be one of the manifestations of:
- thrombocytopenia;
- cryoglobulinemic vasculitis;
- paraneoplastic syndrome;
- sepsis;
- meningococcal meningitis.
Forecast
The prognosis of hemorrhagic vasculitis depends on the form of the disease. In mild cases, in the absence of changes in the kidneys, the disease ends after the first attack with complete recovery. The prognosis becomes worse due to the addition of nephritis, which can become protracted and end in the death of the patient from renal failure.
Severe forms of hemorrhagic vasculitis with confluent ulcerative-necrotic lesions, exposing deeper organs (bones, joints) during tissue disintegration, with intestinal necrosis give high mortality in the first days of the disease.
In rare cases, death occurs from cerebral hemorrhage. The information presented in this article is intended for informational purposes only and cannot replace professional advice and qualified medical care. If you have the slightest suspicion that you have this disease, be sure to consult your doctor!
Forms of hemorrhagic vasculitis
In medicine, this pathology is usually classified depending on the manifestations that accompany its course.
- Skin-abdominal. The organs of the digestive system are affected, pain in the peritoneum is pronounced, intestinal colic often occurs, and a skin rash is present.
- Skin. With the development of this form of the disease, the lesion affects only the skin, on which clearly defined exanthemas of a dark cherry color appear. Most often, the rashes are localized near the joints on the extensor surfaces of the lower (less often upper) limbs and buttocks. Against the background of exanthems, a papular rash also appears, which is often accompanied, for example, by cutaneous-abdominal hemorrhagic vasculitis. The cutaneous form of this disease has a tendency to intense itching in the area where papules and exanthems form.
- Skin-articular. Along with hemorrhagic papules, damage to articular tissues is noted. Most often these are the knee, ankle and elbow joints.
- Renal. In this case, patients experience kidney damage of various origins. There is no skin rash.
Hemorrhagic vasculitis: skin-articular form
The skin-articular form of hemorrhagic vasculitis deserves a separate description - it is characterized by rapid development. Sometimes, before the onset of the disease, a person experiences headaches and general malaise combined with elevated body temperature.
As a result of numerous hemorrhages, small red spots of round shape form on the surface of the skin. More often they merge with each other.
Also, the skin-articular form of pathology is characterized by the appearance of blisters, inflammatory foci, swelling of the skin and soft tissues in the joint area. If the course of vasculitis is particularly severe, the skin-articular form can turn into a necrotic form.
Diagnosis of the problem
Hemorrhagic vasculitis, like other forms of the disease, cannot be diagnosed with a single test. The diagnosis is made on the basis of a comprehensive examination and analysis by the attending physician of a combination of external and internal signs. A blood test is often informative in identifying signs of inflammation. About a third of patients have elevated levels of immunoglobulin A in the blood. If the skin, intestines or kidneys are affected, a biopsy can reveal this type of antibody in the tissue. This is a highly reliable test that helps confirm the diagnosis of this disease. However, negative biopsy results are not a basis for excluding this disease.
Skin biopsies often reveal elevated levels of white blood cells in the skin tissue surrounding damaged capillaries. In the abdominal form of the disease, a CT scan may be required to identify signs of intestinal inflammation.
Symptoms of the lesion
Vasculitis limited to the skin is characterized by the development of small, round red spots (petechiae) and the appearance of reddish-purple areas (purpura). The formation of petechiae is most common in the legs. Purpuric areas represent small hemorrhages under the skin. Other skin lesions associated with rheumatoid purpura include urticarial blisters and necrotizing ulcers, which are usually located on the legs and buttocks. There may be swelling in the face and neck caused by angioedema. Sometimes this can lead to difficulty breathing and can be life-threatening.
Symptoms usually last for several days or weeks. Extensive rashes most often occur on the back of the legs, buttocks, torso and back. Other characteristic signs include painful sensations in the joints, abdominal pain, and sometimes intestinal bleeding. If the kidneys are damaged, protein is present in the urine. If protein loss caused by inflammation in the kidneys is high, swelling of the feet and legs may be present. Various combinations of symptoms are possible, but the most common are skin rashes that accompany the articular, renal and intestinal forms of the disease.
We recommend reading the article on the treatment of vasculitis of the lower extremities. From it you will learn about what vasculitis is, the reasons for its occurrence and methods of treating the pathology.
Features in children
The disease can occur at any age, but children under 3 years of age rarely get it. The greatest number of cases of hemorrhagic vasculitis occurs between the ages of 4 and 12 years.
Features of its course in children are:
- acute onset of illness;
- pronounced exudative component;
- limited angioedema;
- tendency to generalize the process;
- presence of abdominal syndrome;
- tendency to relapse.
In children, hemorrhagic vasculitis is often caused by hypothermia or a severe viral illness. The disease is more often characterized by a fulminant course.
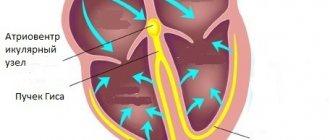
With this disease, children more often than adults experience systolic heart murmurs of a functional nature. In boys with hemorrhagic vasculitis, in some cases, bilateral testicular damage is observed. In half of the cases, children may have no skin manifestations at all.
Children who have suffered hemorrhagic vasculitis are observed by a doctor for another 5 years. They are recommended to have a hypoallergenic diet throughout the year. If the disease occurs with kidney damage, then such observation should continue until adulthood. Such children are not vaccinated for the next 3-5 years.