A hiatal hernia or diaphragmatic hernia is a condition in which some organs of the abdominal cavity are displaced into the thoracic cavity through an enlarged esophageal opening located in the diaphragm. These organs include the abdominal part of the esophagus, stomach, and loops of the small intestine. It is a fairly common pathology; more than half of all cases occur in people over 50 years of age.
Causes
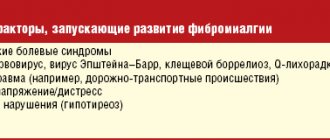
The main predisposing factors to the development of this condition are generally considered to include:
- Weakening of the ligamentous apparatus (decreased elasticity of connective tissue, congenital developmental pathologies).
- Increased intra-abdominal pressure (pregnancy, excess body weight, impaired stool separation).
The main causative factors can be considered:
- Age-related changes in the muscle fibers of the esophagus.
- Reduction in the volume of subdiaphragmatic fat.
- Displacement of internal organs during pregnancy.
- Pathological changes in liver tissue.
- A history of surgical interventions on the esophagus.
- Congenital malformations of the esophagus (shortened esophagus).
- Eating excessively hot food (as a result, burns of the esophagus are observed, resulting in a hernia).
Symptoms
Small hiatal hernias may not show themselves for a long time; as the pathological process progresses, a number of symptoms can be noted.
Heartburn
This is the most common manifestation. Its intensity is entirely variable - from mild to disruptive to the vital functions of the body. Its occurrence is noted after eating, at night, when bending forward.
The main reason for this symptom is the reflux of acidic stomach contents into the esophagus, irritation of the nerve endings.
Pain syndrome
Its occurrence is noted under the same conditions as heartburn.
It can be burning, stabbing, cutting in nature. The most common complaint of patients is retrosternal pain in the hypochondrium, less often in the epigastric region. The basis of the pain syndrome is the retention of food in the stomach with its subsequent reflux into the esophagus.
The pain can radiate to the left shoulder blade, to the left or right arm, to the left half of the neck. Such pain is also characteristic of an attack of angina pectoris, the difference is that the pain is not relieved by nitroglycerin.
Also, the pain syndrome, depending on the complications, may have its own characteristics :
- Compression of the hernial sac at the hernia gate. Characterized by constant dull pain localized behind the sternum or in the epigastrium.
- Strangulated hernia. A sharp, sudden pain appears in the upper third of the abdomen and in the side of the chest where the infringement is localized.
- Solarite. This term refers to an inflammatory process affecting the solar plexus. There is constant and persistent pain in the epigastric region, which is intensified when pressing on the upper abdomen.
- Periviscerite. This is the name given to the inflammatory reaction found in the tissue structures that surround the internal organs. In this case, a rise in body temperature to subfebrile levels (up to 38 C), pain when tapping the anterior abdominal wall, and constant aching pain in the sternum are detected.
Impaired passage of food
There is a violation of the passage of the food bolus even when passing semi-liquid or liquid food. Most often this is accompanied by pain. It can also occur when consuming excessively hot or cold food, or when eating quickly.
Belching
One of the most frequently identified symptoms. Both belching of stomach contents and air may occur. Most often, belching may be preceded by a feeling of fullness in the epigastric region. After the belching passes, the patients’ condition improves significantly, so they often provoke it themselves.
Hoarseness of voice
Associated with a burn of the mucous membrane due to the reflux of acidic stomach contents.
Hiccups
The cause of this symptom is irritation of the nerve endings that innervate the diaphragm, the result is its convulsive contractions.
Cough, heart rhythm disturbances and many other manifestations may also occur.
Why is this hernia difficult to recognize?
It is often really very difficult to suspect a hiatal hernia.
- In half of the cases, the pathology does not manifest itself at all.
- In 35% of cases, the main complaint of patients is interruptions in the functioning of the heart and chest pain, which are often very similar to those that occur with coronary heart disease.
- The majority of patients are elderly people, who usually already have a whole “bouquet” of health problems.
- The presence of a hiatal hernia does not at all exclude the presence of cardiovascular pathology.
All this creates serious diagnostic problems. Many patients continue to undergo treatment with a cardiologist for years, all to no avail, while the actual disease continues to progress.
Diagnostics
Diagnostic measures are based on:
- interviewing the patient (identifying characteristic symptoms);
- instrumental methods (EGD, X-ray examination, pH-metry).
EFGDS
EFGDS – esophagogastroduodenoscopy. It is carried out using a fibrogastroscope. This research method allows us to identify changes in the mucous membrane of the esophagus, the presence of a hernial sac, and a decrease in the length of the abdominal esophagus.
X-ray examination
Allows you to assess the condition of the upper gastrointestinal tract - esophagus, stomach. This is done by injecting a contrast agent (barium). It is possible to identify a part of the organ that has penetrated into the chest cavity, a change in esophageal peristalsis, and incomplete closure of the esophageal sphincter.
pH-metry
Used to determine the frequency and characteristics of reflux of stomach contents into the esophagus. The measurement is carried out during the day, the patient is fitted with a nasogastric tube and a skin sensor. During the study, food intake is allowed (breakfast, lunch, dinner). The sensors read the received data, which is then processed by a special program.
Esophageal hernia: symptoms and treatment, diet, pills
If there is no life-threatening condition - strangulated hernia, severe internal bleeding, when surgical intervention is indicated, treatment begins with conservative measures and includes a whole range of measures.
The patient is advised to avoid wearing tight belts, corsets, and tight belts. To avoid reflux of stomach contents into the esophagus, he needs to sleep with the head of the bed raised, preferably on the right side. Do not overexert yourself mentally and physically, give up alcohol and smoking, and, if necessary, normalize your body weight.
In nutrition, the principle should work, and very strictly, “less is better, but more often.” In other words, you need to eat in small portions 5-6 times a day, and have dinner at least 3 hours before bedtime. Products that can irritate the mucous membrane of the gastrointestinal tract, as well as those that contribute to the development of constipation and gas formation, are excluded from the diet.
As a rule, these are spicy, fatty, fried, smoked dishes, all kinds of canned food, fresh bread, strong tea and coffee, sweets, sour juices, alcoholic and carbonated drinks, cabbage, radishes, peas, grapes... You should approach dairy and fermented milk with caution products.
If they do not cause you bloating, heartburn, or belching, then they are not contraindicated for you. Your menu should include a sufficient amount of fiber, lean meats and fish, and baked apples without peel.
Before and after meals, it is useful to take 1 teaspoon of unrefined sunflower oil, during the day and 1 hour before bedtime to neutralize the acid in the esophagus - half a glass of mineral water "Essentuki" No. 17, "Borjomi" without gas.
After eating, you should never lie down, do bending exercises, or engage in heavy physical work. You need to sit for half an hour, walk around, and best of all, jump lightly for a while.
As for drug treatment, it is primarily aimed at eliminating the main symptoms of the disease - debilitating heartburn, sour belching, discomfort and chest pain after a heavy meal.
These types of manifestations are dealt with well by drugs from the antacid group - Almagel, Gastal, Maalox, Rennie, Gaviscon. They neutralize the effect of hydrochloric acid found in gastric juice, and also have an enveloping effect.
Antacids are taken an hour after meals and before bedtime 3-4 times a day for 3-4 weeks. If you take them longer, diarrhea may develop. On top of this, calcium metabolism will be disrupted and the magnesium content in the blood will increase, which can lead to serious kidney problems.
Enveloping drugs that reliably protect the mucous membrane also include denol (2 tablets in the morning and evening, 15-20 minutes before meals), Venter (2 tablets 3 times a day, half an hour before meals).
The next group of drugs aimed at inhibiting the production of acid in the stomach is the so-called proton pump inhibitors: omez, nexium, pariet, omeprazole, pantoprazole. H2-blockers of histamine receptors, such as ranitidine, famotidine, and nizatidine, can also reduce the secretion of hydrochloric acid.
Eliminate backflow of food and improve its evacuation within the capabilities of prokineticists. These include motilium, raglan, metoclopramide, and domperidone.
I do not indicate dosages and duration of treatment for the reason that in each specific case there will be an individual regimen, which the attending physician will tell you about.
But treat painkillers such as analgin and ibuprofen with caution. In some cases, they are the ones who provoke the reflux of food.
Among the most serious ailments of the gastrointestinal tract, hiatal hernia occupies one of the leading positions. For successful treatment, it is necessary to carry out timely diagnosis and establish an accurate diagnosis.
The type and methods of rehabilitation are selected depending on the stage of the disease, taking into account the general condition of the patient. In combination with medication and surgical treatment, a variety of folk healing recipes are allowed.
After completing the treatment course, a gentle diet is prescribed and sports activities are limited.
The disease has a second name - hiatal hernia. The diaphragm consists of holes that allow nerves, the esophagus and blood vessels to pass through. It separates the sternum and abdominal cavity, holding these internal organs in place.
On the left side of the diaphragm is the digestive system, which in its dimensions should completely coincide with the size of the esophagus.
The reason for the formation is the weakening of the muscle ring, when the viscera are displaced from the peritoneum into the chest cavity, thereby creating a bulging of the abdominal cavity.
In some cases, the disease is congenital (short esophagus).
- Pregnancy;
- Tumor in the sternum or abdomen;
- Having bad habits;
- Consequences of operations on the esophagus;
- Abdominal injuries;
- Constant constipation;
- Cough for a long time.
- Thermal burns caused by eating hot food. They provoke a narrowing of the esophagus, which in many cases leads to a hernia;
- Flatulence;
- Congenital features, for example, a short esophagus;
- Liver atrophy on the left side;
- Weakening of the muscles and ligaments of the esophagus;
- Increased intra-abdominal pressure;
- Esophageal dyskinesia;
- Resorption of adipose tissue located under the diaphragm.
A big role is played not only by the internal characteristics of the body, but also by the person’s lifestyle.
Most often, the disease is diagnosed in the elderly, since with age the human body weakens and the internal organs are no longer so firmly held in their permanent places.
Symptoms
The most common signs of a hiatal hernia are:
- Painful sensations. This is the most characteristic sign of the disease. The pain can occur suddenly and very strongly. Places of occurrence: behind the sternum, “under the stomach”, in the hypochondrium on the left side. Can increase significantly with physical activity and movement;
- Difficulty swallowing, feeling of a lump in the throat. When trying to “swallow” its pain may increase, creating unpleasant sensations behind the sternum;
- Regurgitation, belching of bitter air, can be produced either by air or by food. Upon completion, the patient’s well-being improves;
- Heartburn that occurs on an empty stomach or after eating, while lying down. Leaning your body forward can make heartburn worse;
- Feeling short of air;
- At night, there is an increased secretion of saliva, coughing attacks are accompanied by a feeling of suffocation.
- Dysphagia. It is characterized as the appearance of difficulties when moving both solid and liquid food through the esophagus. This symptom manifests itself more strongly when eating hot or cold food, as well as during its rapid absorption;
- Hoarseness of voice. Its appearance is explained by the release of part of the stomach contents into the oral cavity and larynx;
- Cough. It appears due to pinching of the vagus nerve. It is often associated with suffocation attacks and abnormal heart rhythms;
- Hiccups. It can be quite long, which causes a lot of inconvenience for patients;
- Burning tongue. It is observed quite rarely due to gastric contents entering the mouth;
Some patients may suddenly experience increased blood pressure and hoarseness.
Diagnostics
To make an accurate diagnosis, the patient needs to take the following steps:
- Visit a specialist and describe your pain in detail;
- Take an x-ray to determine the exact location and condition of the digestive organs and also to assess the functioning of the upper gastrointestinal tract;
- Undergo FGDS (Fibrogastroduodenoscopy) - It is carried out using a special movable thin probe with an optical system, with the help of which the stomach and duodenum are examined. It helps identify symptoms that may indicate a possible hiatal hernia and requires special training;
- Measure pH - the level of the esophagus and stomach: during the day, a special device will record the frequency of food entering the esophagus and note all the features of the process.
- Ultrasound of the thoracic and abdominal organs.
The methods used in diagnosis allow not only to establish an accurate diagnosis, but also to determine the severity of the disease.
This subtype includes antral and fundal hernias, which are formed as a result of congenital pathology of the gastrointestinal tract.
Varieties:
- hiatal hernia
- subtotal
- total gastric
- cardiac.
When the position of the patient's body changes, the axial hernia moves freely from the abdominal region to the thoracic region.
Hiatal hernia is dangerous because strangulation often occurs, requiring mandatory surgery.
It received this name because the hernial protrusion moves (“slides”) with each change in the position of the patient’s body.
The size of the protrusion determines the division of the disease into 3 degrees:
- 1st degree protrusion. The esophagus enters the opening of the diaphragm only with a small part of the lower section.
- With degree 2 protrusion, the cardia shifts slightly and the entire lower intestine moves into the patient’s sternum.
- In degree 3, the protrusion involves the fundus and body of the stomach and the lower part of the esophagus.
Treatment options
If a hernia is detected, you must contact a specialist: a gastroenterologist or surgeon. Only they decide how to treat the hernia.
The disease is treatable with medications and surgery.
If the gastroenterologist determines that the symptoms of the disease are moderate, treatment is possible without surgery, with the help of medications, by refusing to eat certain foods and using recommended exercises to reduce the patient’s body weight.
Surgery is inevitable if there is no positive dynamics of drug treatment, or if there is a risk of complications. Urgent surgical intervention is required at the onset of the inflammatory process and in the event of the formation of an esophageal ulcer.
Treatment is carried out mainly in a hospital, where the patient will be constantly under the supervision of specialists.
The operation is prescribed if there is no positive result from medication treatment and there are indications for surgery. If there is a large hole in the diaphragm, surgery is inevitable.
How to treat?
Treatment of this pathology occurs both conservatively and surgically.
Most often, treatment is surgical. It is performed for the following indications:
- Inflammation of the esophageal mucosa, which cannot be controlled by medication.
- The presence of a large diameter hernia, which is accompanied by a violation of the passage of food through the esophagus.
- High probability of hernia strangulation.
- Barrett's esophagus.
- Insufficiency of the esophageal sphincter.
Goals of surgery:
- Restoration of the anatomical integrity of the esophagus and stomach.
- Preventing the reflux of stomach contents into the esophagus.
Pills
For concomitant therapy, conservative treatment is used, which may include the following medications :
- Enveloping agents (Almagel, Phosphalugel, Maalox).
- Proton pump inhibitors (Omeprazole, Rameprozole).
- H2-histamine receptor blockers (ranitidine, famotidine).
What complications does a hiatal hernia lead to?
The more severe the hernia and the longer targeted treatment is delayed, the more the risk of complications increases. The most commonly observed:
- pinching of organs that have moved from their anatomical location by the muscles of the diaphragm;
- reflux esophagitis - inflammation of the esophagus, as a result of constant reflux of the acidic contents of gastric juice, leading to ulcers on the surface of the mucosa, perforation;
- formation of adhesions, scars, narrowing of the lumen of the esophagus;
- stomach ulcer;
- acute or chronic bleeding from varicose vessels of the esophagus and stomach, anemia;
- attacks of angina pectoris, which are difficult to combat with nitro drugs;
- Barrett's esophagus is a precancerous disease.
The likelihood of malignant degeneration of mucosal cells increases
Nutrition
It is imperative to follow an appropriate diet for a hiatal hernia.
The following foods are allowed for consumption:
- dried fruits (dried apricots, prunes);
- fermented milk products with a low fat content (cottage cheese, yoghurts, milk and others);
- lean types of meat and fish (chicken, rabbit);
- crackers, previously soaked in tea or milk;
- slimy porridges, soups;
- tea with added milk.
It is necessary to exclude spicy, fatty, spicy, overly salty dishes and foods, as they overly irritate the mucous membrane of the digestive tract.
Treatment methods
A hiatal hernia can be treated using conservative (non-surgical) methods or surgery.
Non-surgical method
Only small hernias with mild symptoms are treated without surgery. The method is 99% similar to the treatment of gastroesophageal reflux. An important component will be the elimination of bad habits and nutritional correction.
Medication method
Esophageal hernia is treated with six groups of drugs:
- Antacids to neutralize excess hydrochloric acid: almagel, maalox, phosphalugel.
- Prokinetics to restore proper movement of food: cerucal, domirid, motilium.
- Histamine receptor blockers to reduce the production of hydrochloric acid: ranitidine, roxatidine, famotidine.
- Proton pump inhibitors are similar to the previous group, but have lesser consequences: omeprazole, nolpaza, contraloc.
- Bile acids for neutralizing accidentally “abandoned” bile acids: ursofalk, urochol.
Operating method
Surgical treatment is recommended when:
The essence of the technique
Reviews after the article
Meirama pillow
We accept pre-orders.
Order
- severe form, refractory to drug treatment;
- large hernia with poor passage of food or its reflux into the esophagus;
- there is a high probability of strangulation or other complications (narrowing of the esophagus, anemia);
- Barrett's esophagus;
- paraesophageal hernia.
The operation is necessary to restore the anatomy of the stomach and esophagus, providing an anti-reflux mechanism to prevent the reflux of food.
Surgical intervention is contraindicated for pregnant women, with severe forms of cardiovascular diseases, oncology, diabetes mellitus, and thrombophlebitis. There are several types of operations depending on the method of access to the hernial sac. The cost of surgical treatment is determined by numerous factors and individual patient characteristics:
| Type of operation | Cost, rub. |
| Nissen fundoplication | 50 000 – 150 000 |
| Operation Belsey | 70 000 – 90 000 |
| Hill gastrocardiopexy | 80 000 – 160 000 |
| Allison technique | 50 000 – 100 000 |
Video
Professor K.V. Puchkov will talk about the surgical method of treating a hernia, features of the postoperative period and methods of treating heartburn in case of an esophageal hernia:
Nissen fundoplication
It can be performed using the open method or using a laparoscope. A cuff is created on the upper third of the stomach, which prevents stomach contents from entering the esophagus. Next, the upper part is lowered and the legs of the diaphragm are sewn together. This allows the hole diameter to be reduced. The operation is contraindicated for narrowed esophagus, impaired motility and inflammation.
Flaws:
- The long course of the disease shortens the esophagus, which does not allow it to descend. Then part of the stomach remains in the chest, which can cause a relapse.
- The cuff is not fixed and may come off. The disease will begin to develop again.
Advantages:
- You can use laparoscopy, which will ensure minimal trauma and reduce the recovery period.
- Low risk of developing postoperative complications.
Operation Squirrels
Indicated for large hernias and obvious reflux esophagitis. The doctor makes an incision on the left side in the 6th intercostal space. The lower part of the esophagus, the sphincter, is secured to the diaphragm. In addition, the fundus of the stomach is sutured to the wall of the esophagus. The disadvantages of the method are access to the hernia. The surgical incision causes severe pain and is difficult for patients to tolerate. However, the operation will help eliminate concomitant pathologies in the chest cavity.
Gastrocardiopexy
A laparotomy is made - an incision in the middle of the abdomen. Surgeons suture the upper third of the stomach and esophagus to certain structures (greater omentum, round ligament of the liver, etc.).
The most common gastrocardiopexy according to Hill, when there is a strong fixation of part of the stomach, esophagus to the middle ligament of the diaphragm and preaortic fascia.
During surgery, doctors have difficulty finding the preaortic fascia and medial arcuate ligament.
Allison technique
The legs of the diaphragm (hernial orifice) are sewn in. An incision is made in the eighth or seventh intercostal space. After surgery, there is a high probability of relapse - 10%. The gastroesophageal reflex will not be eliminated. Today, the method is not used independently, only in combination with other methods of surgical intervention.
Read how to treat a diaphragmatic hernia in children and adults here.