The health and life of the unborn baby depends on a huge number of factors.
Heredity plays a role, as does the mother’s behavior during pregnancy, her diet, daily routine, the presence of infectious diseases, and congenital developmental abnormalities.
But not all pregnant women know that the success of bearing a child depends on the nature of the attachment of the fetus to the wall of the uterus.
Most often, expectant mothers who are faced with a diagnosis of chorion presentation find out about this.
What is chorion
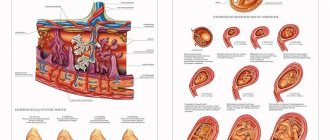
Chorion is one of the membranes that surrounds the baby in the uterus and provides communication with the mother’s body. This structure provides nutrition and breathing to the child, as well as the removal of its metabolic products.
It is also a kind of barrier that protects the small organism from harmful influences.
The period of active functioning of the chorion is the first trimester, later it is replaced by the placenta, which will ensure the connection between mother and child until the moment of birth.
How the chorion attaches to the wall of the uterus
The chorion has many outgrowths called villi, which are embedded in the wall of the uterus. They are penetrated by a dense network of capillaries and come into contact with the mother’s blood vessels.
Normally, the chorion is attached to the fundus of the uterus or its walls in the upper part.
This arrangement is the most favorable: when the uterus stretches during the baby’s growth, neither the chorion in the first trimester nor the placenta in subsequent stages will be damaged or peeled off, and the blood vessels will maintain integrity and ensure uninterrupted nutrition and breathing of the baby.
Fertilized egg on ultrasound: sizes by week of pregnancy
The fertilized sac is a round or ovoid (egg-shaped) formation that surrounds the embryo, usually located in the upper half of the uterine cavity.
In the early stages of pregnancy (in the first trimester), an ultrasound examination is performed to determine the localization (location) of the fetal egg. On an ultrasound, the fertilized egg looks like a small dark gray (almost black) spot with clear contours.
The presence of a fertilized egg in the uterine cavity eliminates the possibility of an ectopic pregnancy. In a multiple pregnancy, you can see two separately located fertilized eggs.
What is chorionic presentation
In some women, the chorion is attached to the lower part of the uterus. In this case, they talk about presentation. Based on the nature of its localization, they are distinguished:
1 Low position
– the chorion is attached to the lower segment of the uterus, but does not block the cervical canal (that is, it does not block the path along which the baby will move during childbirth).
In this case, severe bleeding may occur, feeding and breathing of the fetus becomes impossible. Recommended.
3
Constant disruption of the connection between the placenta and the maternal body can cause fetal hypoxia (oxygen starvation), delayed growth and development, and in severe cases, death.
4
Although a low-lying placenta is considered the least dangerous for mother and baby among all presentation options, it can cause complications during labor.
5
With complete placenta previa, natural childbirth provokes heavy bleeding, which can lead to death of the mother and fetus.
Therefore, a caesarean section would be the only reasonable solution.
6
In case of complete and partial presentation, vaginal examination is not recommended during a gynecological examination, as it can cause bleeding.
Thus, placenta previa, especially complete one, is a truly dangerous phenomenon that causes a lot of difficulties.
But if this problem is detected on time, in the early stages of pregnancy, a woman has a high chance of having a healthy baby. However, control over the condition of the expectant mother and her child should be more careful.
Interesting! Fourth month of pregnancy: development continues
13th week of pregnancy for the expectant mother
For the expectant mother, the 13th week of pregnancy is a reason for happiness and joy, a third of the term is over, toxicosis has passed, irritability has passed, and it is even possible to determine the sex of the unborn child. This is the perfect time to enjoy all the delights of pregnancy. At this stage of pregnancy, a woman’s belly begins to appear. Although it is still invisible to others, the woman already feels the tightness of her usual clothes. The 13th week of pregnancy is the best time to update your wardrobe.
When the thickness of the chorion at 13 weeks corresponds to the number of weeks of pregnancy, and the placenta has already begun to perform its functions, a woman needs to be extremely careful in choosing foods, especially sweets and starchy foods, which can only lead to excess weight for both mother and child . It is better to start eating fresh berries, vegetables and fruits. In this case, it is necessary to monitor the intake of all necessary substances into the body.
Particular attention should be paid to calcium, which is very important in the 13th week, so you need to start taking green vegetables, apples, persimmons, kiwi and lentils. These products are extremely important for proper metabolism between the placenta and the child, because at 13 weeks of pregnancy we can say that the normal thickness of the chorion is the thickness of the placenta.
At this stage, a pregnant woman should start using creams for stretch marks and pay special attention to the breasts, abdomen, hips and buttocks. The time has come to devote all your time to caring for your loved one. After all, it is during this period that a pregnant woman is especially feminine and beautiful!
Causes of chorionic presentation
The doctor may not be able to determine the factor that played a decisive role in the incorrect location of the placenta. The most common causes of presentation are:
1
Congenital anomalies of the structure of the uterus, scars and defects in its wall, which arise due to previous surgical operations, cesarean section or frequent inflammatory processes.
2
Presentation occurs more often in women who have a large number of children, or in those who encountered this problem during a previous pregnancy.
3
A woman's age over 35 years is also a risk factor; the likelihood of placenta previa increases if the woman has bad habits (smoking is especially dangerous).
What awaits a pregnant woman if she is diagnosed with chorionic presentation
The expectant mother should be aware that in the case of placenta previa, she must be more careful and attentive. Most likely, you will have to spend some time in the hospital.
Some women with this diagnosis are forced to spend quite a long time in the hospital, but the health of the child is more important, so you will have to be patient.
This diagnosis cannot be eliminated by treatment. If the placenta itself does not change its location during pregnancy, then no external factors will be able to influence it.
All medications that are prescribed to a woman for breech presentation are designed to eliminate complications (for example, stop bleeding) or support the condition of the mother and her baby (multivitamins are often recommended, which can reduce the risk of decreased development).
Throughout pregnancy, a woman should follow a more gentle daily routine, rest more, and avoid physical and mental stress that can cause bleeding. Sexual contacts are often prohibited. If bleeding occurs, bed rest is recommended.
During pregnancy, many things frighten the expectant mother. The words about the attachment and presentation of the chorion at the first ultrasound sound especially scary. In most cases there is nothing to fear. But some situations require careful follow-up and treatment.
The fertilized egg with the embryo developing in it consists of two membranes. The chorion is the external one, which at 12-14 weeks turns into the placenta.
A feature of the structure of this structure is the abundant amount of villi on the surface. With their help, the fetus is attached to the wall of the uterus. This is an important stage affecting a normal pregnancy.
Chorionic detachment and hematoma
A hematoma due to chorionic detachment is not so dangerous if it occurs at the beginning of pregnancy and is not of a large scale. With partial detachment of the chorion, a retrochorial hematoma is usually formed. It is clearly visible during ultrasound diagnostics. If it is small and there is no circulatory disturbance in the child, then there will be no bleeding during chorionic detachment. However, a number of measures will still have to be taken to normalize the situation. With properly prescribed therapy, placental abruption stops, and the pregnancy continues to develop normally. The placenta will grow over time, which will compensate for the area where this hematoma occurred. In this case, the baby’s health is not in danger. Such a favorable development of the situation can only occur during the first trimester.
If this diagnosis is made at a later date, then the child will hardly be able to cope without oxygen starvation.
Here you will have to go to the hospital and be there under the constant supervision of doctors, follow all their instructions and recommendations.
Medicines for expectant mothers: what can pregnant women take for headaches?
How to relieve swelling during pregnancy? Find out here.
How to cure a cough in a pregnant woman: .
Types of chorion attachment, some features
The uterus is conventionally divided into three parts: the lower segment, the anterior and posterior walls. When the chorionic villi attach to one of them, the full development of the embryo and placenta begins. There are the following types:
- Along the front wall.
- On the back wall.
- Bottom view.
If the chorion is on the back wall of the uterus, then this is not a pathology, but the most favorable development option. This is related to:
- good blood supply to the area;
- low stretchability;
- the absence of mechanical impact on the fetus when it moves its legs.
Doctors also regard the localization of the chorion along the anterior wall as a variant of the norm. Pregnant women with this diagnosis are included in the high-risk group for bleeding. They are given general recommendations and are not prescribed medication.
Be sure to visit a specialist on an individual schedule!
When treating pregnant women with chorion located on the anterior wall of the uterus, doctors may encounter some difficulties:
Such problems can be easily solved through in-depth monitoring, including more frequent ultrasound and tocography (the baby’s heartbeat is assessed).
Attachment of the chorion in the lower segment of the uterus is a prognostically unfavorable sign. If it is located more than 3 cm above the cervix, then the pregnant woman is treated on an outpatient basis with more careful dynamic monitoring. It is worth considering that such terminology is appropriate only for very short periods. After 12 weeks they talk about placenta previa.
Chorionic thickness by week of pregnancy: table
The first ultrasound examination is carried out at approximately 12 weeks.
During the examination, the attachment of the organ is assessed, which may differ and is not pathological. In this case, presentation is diagnosed along the posterior or anterior wall of the uterus, less often a low chorion is recorded, and subsequently migration of the organ to the side walls often occurs. Additionally, the chorion structure and thickness are assessed. Initially, the most thickened section of the chorion, which is approximately equal to the number of weeks of gestation in millimeters, is subject to measurement by ultrasound. The table shows the normal limits for membrane thickness in early pregnancy:
| Gestation period, week | Thickness of the chorion (placenta), millimeters |
| 7 | 7-14 |
| 8 | 8-15 |
| 9 | 8,5-16,5 |
| 10 | 9,5-17,5 |
| 11 | 10-18,5 |
| 12 | 11-20 |
| 13 | 11,5-21 |
| 14 | 12,5-22 |
| 15 | 13-23 |
| 16 | 14-24 |
Significant thickening of the chorion is observed in diabetes mellitus or with the development of hemolytic disease, while thinning indicates placental insufficiency and premature aging, which leads to spontaneous miscarriage.
Chorionic presentation: what is the danger?
Attachment of the chorion is a natural process necessary for the further good development of the embryo. Against this background, a situation may arise when the fertilized egg is located very low (close to the internal os, less than 3 cm), covering the natural birth canal. This condition is called chorion presentation. The following types are distinguished:
- marginal;
- central;
- incomplete (partial).
Regional presentation is considered more successful. In this case, the chorion touches the area of the internal os and the cervix. As the fetus grows and the uterus enlarges, the placenta may migrate. At an ultrasound scan at 18 weeks, this situation usually changes to a normal location.
With central presentation, the chorion completely blocks the cervical canal. This is the most dangerous type, in which massive bleeding often develops and fetal death occurs.
Partial presentation is characterized by the fact that the chorion covers the lumen of the cervical canal by 2/3 or less. The advantage of this type is that when the placenta migrates, it moves to the marginal localization, and then to the normal position.
The danger of any kind lies in the possible occurrence of complications. These include bleeding of varying degrees of intensity and antenatal fetal death. If medical care is not provided in a timely manner, a woman’s life is at risk. Such complications are due to the development of a good blood supply system when the fertilized egg is attached to the uterine wall.
As a result of certain factors (intense physical activity, high blood pressure, uterine hypertonicity), a slight detachment of the chorionic villi occurs, which is accompanied by the development of bleeding. Depending on the area of the damaged area, it will vary in intensity.
Types of chorion
Medicine knows several varieties of the upper membrane of the fertilized egg. It is worth noting that they all depend on the stage of pregnancy and can change greatly over time. The type of chorion can only be determined by ultrasound examination.
Gestation period up to 6 weeks from conception
At this stage of development of the fertilized egg, a ring-shaped chorion can be detected. What it is?
During examination using an ultrasonic sensor, a fertilized egg can be detected. It is worth noting that the embryo is not yet visible at this stage. The upper membrane of the fertilized egg is attached to the endometrium over its entire area. It is in this case that we can say that there is a ring-shaped chorion.
Gestation period up to 8 weeks from conception
Often in the ultrasound examination report, women find the entry: “Circular chorion.” What does it mean?
This condition of the upper membrane is characteristic of early pregnancy. This type of formation is transformed approximately at 8 weeks from the moment of fertilization.
This type of shell is absolutely normal. Many women ask their gynecologist: “Villous chorion: what is it?”
The shell got its name because it has so-called villi. It is with their help that it is attached to the inner wall of the reproductive organ. Villous chorion is always described in the ultrasound report. Its location is also noted.
Causes of presentation, diagnosis and treatment
The true reason for the development of such situations has not yet been found. Background factors for the occurrence of presentation are:
The only method for diagnosing chorionic attachment and presentation is ultrasound! It is carried out in the early stages, when it is already possible to diagnose abnormalities and prevent the development of complications.
Pregnant women with central chorionic presentation must be hospitalized in a specialized hospital. It is impossible to cure this condition! The actions of doctors are aimed at preventing the development of complications. Therapy for all patients is comprehensive. It includes general recommendations and prescription of medications. A positive result largely depends on the pregnant woman herself.
Drug therapy is aimed at reducing uterine tone, pressure, and treating stress. Antispasmodics include No-shpa in tablets, Papaverine in rectal suppositories, Magne B6, and ginipral. The dose, duration of use and specific medicine are selected by the doctor!
It is possible to carry and give birth to a child with different localizations of the chorion. Many girls give birth naturally without any complications. If placenta previa persists, delivery is carried out by planned cesarean section. This is done to prevent complications during childbirth and preserve the life of the mother and baby.
During a routine ultrasound examination, which is carried out after the 12th week of pregnancy, among other factors, the functional diagnostics doctor pays attention to the position of the chorion. In most cases, this parameter does not cause any concern to the specialist. However, there are situations when the expectant mother is diagnosed with chorionic presentation. Is this phenomenon dangerous? What types of chorionic presentation are there? Which of them require therapeutic measures? How is chorionic presentation diagnosed and treated?
Localization of the chorion
There are several common options for attaching this structure. Doctors still do not know why the fertilized egg chooses this or that place. Let's look at each possible option.
This condition is the most common. In most cases, in the first trimester of pregnancy, chorion is detected along the posterior wall of the reproductive organ. In this case, it is necessary to take into account the structural features of this shell.
If your chorion is not located along the back wall, then it is attached to the front of the uterus. This condition is also normal, but special precautions must be taken.
What is chorion: its structure, functions and connection with the placenta
The chorion is the outer membrane that surrounds the embryo and is its connecting link with the mother’s body. Its formation begins after the second week of pregnancy. The chorion is attached to the inner wall of the uterus with the help of villi. Its structure is presented in the form of a white ring with wavy outlines, located on the outer edge of the fertilized egg.
Without chorion, the vital activity of the fetus is impossible. This is because through this shell:
- gas exchange occurs between the embryo and the pregnant woman;
- excretory and trophic functions are carried out;
- the child is protected from the negative influence of pathogenic agents.
If in his conclusion the functional diagnostics doctor indicates that the structure of this organ has not been changed, the process of bearing a child proceeds in a standard manner. Otherwise, disruptions in the course of pregnancy occur.
The chorion retains its ring-shaped form until 9 weeks of gestation. Then its structure changes, it becomes smooth and branched. After this, the placenta is formed from the chorion. This happens after 13 weeks of pregnancy.
What is chorionic detachment during pregnancy and how to identify it?
During pregnancy, a special system develops in the mother’s body that allows the child to receive all the substances necessary for development. The main component of this system is the chorion or placenta. Through it, nutrients are supplied to the baby.
Most of the waste generated during the life of the fetus returns to the mother's body through the general bloodstream. All excess and harmful substances are excreted along with urine.
Placental abruption often occurs at different stages of pregnancy. If this happens in the later stages, it may cause urgent delivery. During the first trimester of pregnancy, a fully formed chorion is not observed. Here the so-called villi are formed so that the fertilized egg is firmly anchored in the mother’s body.
A woman herself can determine chorionic detachment based on characteristic symptoms:
1. Bleeding from the vessels of the uterus;
2. Severe pain in the lower abdomen
Doctors distinguish three key types of this diagnosis:
- Light form. It usually does not make itself felt in any way, so the diagnosis can only be revealed by ultrasound examination.
In some cases, even ultrasound does not help determine the presence of such a defect, and it is diagnosed after childbirth, when minor blood clots are observed on the surface of the placenta;
- Medium shape. With it, the woman feels discomfort in the lower abdomen and notices slight bleeding, but chorionic detachment can occur without them - this moment is directly related to the size of the hematoma and the area where it occurred. If you palpate, you can feel the tense uterus. The baby may experience an irregular heartbeat - this indicates a lack of oxygen;
- The severe form is associated with severe pain. The woman feels that her stomach is bursting with pain, she begins to feel dizzy, her heart beats faster, her blood pressure and temperature drop.
Location in the uterus
Dear reader!
This article talks about typical ways to solve your issues, but each case is unique! If you want to know how to solve your particular problem, ask your question. It's fast and free
!
The chorion can occupy different positions in the uterus. The most favorable localization is considered to be its attachment to the fundus of the uterus or its walls in the upper region. This arrangement prevents damage and detachment of the chorion and placenta during the stretching of the uterus during fetal growth, and also prevents damage to the integrity of the vessels that are responsible for the delivery of nutrients and oxygen to the embryo.
During pregnancy, the location of the organ may change. This phenomenon is called migration. In situations where the chorion is not properly attached to the walls of the uterus, we are talking about presentation.
The phenomenon in which this organ is located in the lower part of the uterus and partially or completely blocks the pharynx of the cervical canal that passes into it is considered conditionally pathological.
What it is
The chorion is a temporary organ that performs the functions of a pharmacist. It is formed from the moment the fertilized egg is implanted from the fallopian tube, where the egg and sperm meet, into the uterine cavity. As soon as the blastocyst (which is what the fertilized egg turns into by 8-9 days after ovulation) reaches the uterine cavity, it strives to gain a foothold in it. It is this process that is called implantation.
At the site of attachment of the blastocyst shell, special enzymes are secreted that make the mucous membranes of the uterus more pliable and allow the fertilized egg to “grow.” A chorion is formed at the site of attachment. It is necessary to supply the fertilized egg with useful substances from the mother’s blood. A little later, the placenta appears in its place. But until the 12-13th week we are talking specifically about the chorion, since the placenta is still forming and does not function.
If implantation is successful, the fertilized egg is fixed in the fundus of the uterus (this is its upper part). If, for some pathological reason, the blastocyst fails to implant in the upper or middle part of the uterus, it may descend into the lower uterine segment. And then the chorion will form low.
Chorionic presentation refers to its location relative to the cervical canal, a thin passage inside the cervix that connects the uterine cavity and vagina. There is no talk of presentation only if the chorion has formed in the area of the fundus of the uterus or in its middle part (in the body of the uterus).
If the chorion is low, there are several types of presentation.
Types of chorion presentation during pregnancy
Previa of the future placenta occurs:
- Full (central). It completely covers the opening of the cervical canal. When diagnosing such an arrangement of the villous membrane of the fetus, in the vast majority of cases, immediate hospitalization is indicated.
- Incomplete. This type is divided into partial and marginal presentation of the chorion. In the first case, the overlap of the pharynx is determined by 2/3. With marginal presentation of the chorion, the third part of the internal os is covered by the membranes of the embryo, and the edge of the future placenta is located on the periphery.
- Low. The villous membrane of the fetus is located less than 3 cm from the pharynx, and the situation does not reach its complete overlap.
There are also such types of chorion localization as:
- Rear. If the doctor’s report on functional diagnostics includes the phrase “predominant localization is posterior,” you should not be alarmed. Chorion on the posterior wall is not a pathological phenomenon. Here we are talking about one of the most common types of fastening of this organ.
- Front. If the future placenta is not located on the back wall of the uterus, then it is attached to the front. This localization is considered normal, but requires observation. If precautions are not observed, the anterior type of attachment of the chorion is fraught with detachment of the membranes of the embryo.
- Side. We are talking about a side position. It always comes down to the front or the back. In this case, the conclusion of the study will indicate that the chorion, for example, is located behind and to the right.
Types of presentation
To assess the position of the chorion, doctors focus on its position relative to the os (the place where the uterus meets the cervix). If it is more than 3 centimeters away from this anatomical landmark, then the placenta develops normally. In other cases, the following classification is used:
1. Central complete chorion presentation.
It is characterized by the fact that the fetal membrane completely covers the internal os of the uterus. This type of presentation is the most unfavorable.
2. Central incomplete chorion presentation.
Sometimes it is called partial. This presentation is characterized by the fact that the chorion touches up to two-thirds of the uterine pharynx. Has a better prognosis.
3. Regional presentation of the chorion.
It is a variation of the previous one, but some doctors distinguish it into a separate category. With this type of pathology, the placenta develops, affecting less than one third of the uterine os. Regional presentation of the chorion at 12 weeks is a relatively favorable option for the fetus, since in half of the cases the membrane will take a physiological position after a certain period of time.
4. Low chorion presentation.
With this type of abnormal position, the placenta is formed outside the uterine os, but it is located at a distance of 3 or less centimeters from it. Low presentation is a fairly favorable diagnosis; in 90% of cases, by the end of pregnancy, the membrane occupies a normal place in the organ cavity.
Some experts distinguish anterior and posterior chorionic presentation, when the structure is formed on the anterior or posterior wall of the uterus, respectively, but is located at a distance of more than 3 centimeters from the pharynx. These conditions of the membrane are absolutely normal; over time, the placenta will move to the bottom of the organ.
An accessible explanation about “Placenta Previa” by obstetrician-gynecologist S.M. Dyakova:
Symptoms and diagnosis
There are no signs that would directly indicate an abnormal location of the future placenta (marginal, partial, complete, low). The pathological course of gestation can be determined only by a number of indirect manifestations:
- bleeding;
- occasional spotting;
- weakness;
- attacks of dizziness;
- clouding of consciousness;
- pulling or cramping pain in the lower abdomen.
This pathology can be detected only after 12 weeks of gestation. In modern medicine, chorionic presentation at 13 weeks can be diagnosed exclusively using ultrasound.
How are they treated?
The main task in case of chorionic presentation is to take measures to maintain pregnancy. In case of heavy bleeding, when conservative methods of therapy are powerless, emergency delivery is resorted to. The table contains information about what procedures are provided for placenta previa.
| Methods for maintaining pregnancy if the placenta is located incorrectly | Drugs used | Purpose of use |
| Medication | Papaverine (rectal suppositories), tablets Drotaverine, Nosh-Pa, Duphaston, Utrozhestan | Decreased uterine tone |
| Vitamin complexes | Strengthening the immune system, improving metabolic processes in the body | |
| Iron-containing medications (Totema, Maltofer, Ferrum-Lek) | Preventing and eliminating signs of anemia | |
| Sedatives (valerian tincture, motherwort tincture) | Relief of psycho-emotional disorders | |
| Hemostatics (sodium ethamsylate) | Stop bleeding | |
| Non-drug | Bed rest | |
| Limiting physical activity. Sudden movements, lifting heavy objects, and playing sports are prohibited. | ||
| Complete sexual rest | ||
| Avoiding stress | ||
| Using a bandage in late pregnancy | ||
| A balanced diet, excluding foods that can lead to disruption of the bowel movement process | ||
The pregnancy process is a very delicate chemistry that affects the entire female body. In order for a child to grow up, you need to take good care of yourself, eat well and not miss doctor’s examinations.
Not all women know what is happening in the world, and this is a rather important point. Every month, a follicle matures in the female body, which ruptures and releases the egg. This period is considered the most favorable for conception. During fertilization, the egg moves through the tubes and enters the uterus, where it is firmly attached to her body. There it develops for quite a long time. Localization of the chorion, chorionic detachment and its presentation can cause a number of problems during the preservation of the fetus and its birth.
What is chorion and what is its role
Throughout pregnancy, the embryo develops in a membrane that protects it from external damage and contains the nutrients the baby needs. Composition of the membrane: amnion and chorion. Where the outer part is the main one, as it is attached to the reproductive organ. Localization of the chorion, chorion detachment is one of the many problems encountered during pregnancy.
This matter is vital for the normal development of the fetus. The chorion appears at the very beginning of the period and exists until that moment. The correct location of the chorion and its uniform distribution are important. It should be located on the back wall of the uterus. Chorionic presentation is when it is located in the lower part of the reproductive organ.
To diagnose problems in this area, it is necessary to carry out, since a simple gynecological examination will not give results.
Types of chorion depending on the duration of pregnancy
Chorionic presentation may occur at different stages of pregnancy. Its location is shown by ultrasound. At 6 weeks, the fertilized egg is usually attached in a ring shape over the entire area. At the 8th week it becomes circular.
Most often, chorion presentation is detected at 12 weeks, since at this time the first planned ultrasound examination is performed. This pathology requires bed rest and hospital treatment. If the placenta rises up, the threat will be eliminated. Chorionic presentation at 12 weeks can only be eliminated through drug treatment. Also, pregnant women are prescribed complete rest and...
Expectant mothers are wondering about chorionic villi: what is it and are they normal. The outer membrane of the fetus has small villi that help attach it to the wall of the uterus, so this structure of matter is considered completely normal.
Localization of the chorion
Experts determine several main positions of placenta concentration:
- Localization of the chorion along the posterior wall. This location of the tissue suggests less deviation from the norm than others.
- The predominant anterior localization of the chorion is a deviation from the norm that requires medical intervention.
- When the chorion blocks the internal os, not only the development of the fetus is hampered, but also its birth.
All problems associated with incorrect presentation can only be solved medically. Women should not resort to traditional methods of treatment.
There are several places where amniotic tissue attaches to the uterus and they all require separate consideration. Localization of the chorion along the posterior wall is most common. This condition is typical in early pregnancy. The primary localization of the chorion is considered to be in the posterior part of the reproductive organ. It is clearly visible during ultrasound examination. In this case, there is no need to panic. The posterior localization of the chorion will not and will not cause spontaneous abortion. The state of matter may change, so specialists prescribe an examination in the early stages. Expectant mothers must clearly understand that the posterior localization of the chorion is a normal development of pregnancy. Usually, in this case, there are no problems with the health of the woman and the unborn child.
The chorion can be located along the anterior wall of the uterus. Experts consider this arrangement of matter to be normal, but warn that expectant mothers should be extremely careful. Chorion along the anterior wall of the uterus can threaten placental abruption, so you must follow all doctor’s instructions. However, this is not a reason to panic, since matter has a specific ability to migrate. Chorion along the anterior wall is not a death sentence, but minor complications that can be eliminated.
Some women experience attachment of the amniotic sac to the side of the reproductive organ. In this case, doctors say: chorion on the front wall or on the back, and on the right or left. This is also determined by ultrasound. Anterior localization of the chorion with lateral deviation is also not a pathology and can change.
The examination results sometimes contain information about the different location of the site of attachment of matter to the wall of the uterus. The low location of the chorion means that the attachment site is in close proximity to the cervix. The distance separating them is no more than 3 centimeters. Low location of the chorion is not a pathology. It is completely acceptable for medical reasons. Low chorionic attachment may change. The uterus enlarges with the growth of the fetus, so the insertion site rises upward. Low chorion attachment can be considered normal if it does not close the pharynx.
There are several types of presentation that are detected by ultrasound.
- Regional chorion presentation;
- Partial;
- Complete.
Complete presentation means that the matter is localized near the cervix and closes the exit for the fetus. The chorion blocks the internal os and interferes not only with spontaneous childbirth, but also threatens arbitrary termination of pregnancy. This may lead to surgery during childbirth. Medicine has not yet developed a way to solve the problem when the chorion blocks the internal pharynx. But experts advise complete rest and proper nutrition for this diagnosis.
With partial closure, one part of the cervix remains open.
The marginal presentation of the chorion involves minimal closure of the exit from the canal and only along one edge. This problem does not contribute to miscarriage, unlike the other two.
Chorionic villus biopsy and indications for it
Many women wonder why a chorionic villus biopsy is performed. You should know that this matter has the same genetic structure as the fetus. In this regard, the procedure can be carried out in order to detect diseases in early pregnancy.
Chorionic villus biopsy is performed for the following indications:
- Late pregnancy;
- Previously born children have diseases associated with chromosomes;
- The genes contain these diseases;
- Echography indication.
Chorionic villus sampling can have complications. This is bleeding, pain or miscarriage. In this regard, the duration of the procedure should not exceed 12 weeks.
Chorionic villus biopsy has its contraindications. If a woman has chronic diseases in the acute stage, the material is not available, there are visible deviations from the norm in the cervix, the presence of fibroids, bloody discharge and other equally serious indications, the procedure is not performed.
Chorionic villus biopsy reviews are quite contradictory. First of all, you need to know that this is a small but painful operation. The procedure is performed through the cervix or abdominal cavity, depending on the location of the matter. In addition, certain complications may arise as the pregnancy continues. No matter what reviews a chorionic villus biopsy has, it should only be carried out due to urgent need and medical indications. The operation is performed under constant ultrasound monitoring.
During the mandatory ultrasound after 12 weeks, the location of the chorion is assessed, among other things. Sometimes an ultrasound specialist diagnoses chorionic presentation. What does this mean and how dangerous is it?
Sonographic markers of miscarriage in the first trimester
Accuvix-A30
Time-tested!
Ultrasound system for conducting examinations with expert diagnostic accuracy.
Introduction
Among the most important problems of practical obstetrics, one of the first places is miscarriage. Premature birth is the most common complication of pregnancy, and prematurity is one of the main causes of perinatal morbidity and mortality.
Despite certain advances achieved in diagnosis, therapy, and prevention of this complication, the incidence of premature birth has increased by 9% in the last five years [1]. Perinatal mortality during premature births is 25 times higher than during timely births, stillbirth rates reach 50%, and early neonatal mortality rates reach 70% [1, 2].
The frequency of spontaneous miscarriages in the first trimester remains stable for many years and accounts for 15-20% of all wanted pregnancies. In the structure of obstetric complications, this pathology ranks second [3]. In this regard, it is necessary to create a diagnostic algorithm for patients with miscarriage for timely optimization of management tactics in the first trimester. The ultrasound method occupies a leading place in the structure of complex diagnostics of this complication, being a highly informative, non-invasive, safe diagnostic test [4-6].
The purpose of this work is to determine the most informative echographic markers of miscarriage in the first trimester to predict pregnancy outcome.
Materials and methods
The main group consisted of 128 women with threatened and incipient spontaneous miscarriage at a period of 8-13 weeks, who were in the miscarriage department of the Perinatal Center of Krasnodar. The studies were conducted before the start of complex therapy.
In the first trimester of pregnancy, ultrasound diagnostics were carried out using two standard techniques, the most informative of which was transvaginal echography, as well as transabdominal scanning techniques with a full bladder. All studies were carried out on modern ultrasound machines using a 6.5 MHz transvaginal probe and 3.5 and 5 MHz convex probes in two-dimensional echo mode; Doppler examination was also used in pulsed and color modes.
Research results
For the first trimester of pregnancy, the following main echographic criteria for threatened and incipient spontaneous miscarriage were used, which were conditionally divided into three groups:
Sonographic signs of pathology of extraembryonic structures
- Amnion hypoplasia was detected in 6 (4.7%) pregnant women. Hypoplasia was considered to be the diameter of the amniotic cavity less than 10-12 mm; the measurement was carried out in two mutually perpendicular planes during longitudinal scanning.
- Chorionic hypoplasia was detected in 8 (6.25%) pregnant women. Normally, the maximum thickness of the chorion corresponds to the gestational age or lags behind it by 2-4 mm. A lag in chorion thickness of more than 5 mm was considered hypoplasia. The measurement was carried out three times in the middle third of the chorion (Fig. 1).
- Fragmented chorion was detected in 2 (1.56%) pregnant women. In the structure of the fragmented chorion, anechoic structures of irregular shape, 5-10 mm in size, are visualized (Fig. 2).
- Branched chorion presentation was detected in 14 (10.9%) pregnant women. In this case, the chorion partially or completely covers the area of the internal pharynx (Fig. 3).
- Leveling of the echogenicity of three extraembryonic cavities (chorionic, amniotic and yolk sac cavity) was detected in 2 (1.56%) pregnant women. Normally, due to differences in biochemical and cellular composition, the contents of the chorionic, amniotic cavities and the yolk sac cavity have different echogenicity [5]. During primary infection, as a result of a pronounced proliferative-exudative reaction of the amniotic membrane and yolk sac, the echogenicity of these cavities increases.
Rice. 1.
Pregnancy 8-9 weeks. Chorionic hypoplasia. The maximum thickness of the chorion is 5 mm.
Rice. 2.
Pregnancy 12 weeks. Fragmented chorion.
Rice. 3.
Pregnancy 10 weeks. Chorionic presentation.
Sonographic signs of pathology of the embryo and ovum
- Deformed ovum, this sign was detected in 35 (27.3%) pregnant women.
- Low position of the ovum occurred in 2 (1.56%) pregnant women. The low percentage of detection of this sign is associated with gestation periods of 8-13 weeks, at which the fertilized egg occupies most of the uterine cavity.
- Retrochorial hematoma was detected in 12 (9.4%) pregnant women. The nature of the localization of the hematoma (polar or parietal) and the time of its formation (echographic signs of hematoma organization) are important (Fig. 4 a, b).
- Fetal bradycardia (heart rate less than 90 beats per minute) was detected in 2 (1.56%) pregnant women. The fetal heart rate was determined using spectral Doppler.
- Early oligohydramnios was detected in 4 (3.1%) pregnant women. Inconsistency between the diameter of the fetal egg and the gestational age. The measurement was carried out in three mutually perpendicular planes, along the internal contour of the fetal egg.
- Impaired differentiation of the main anatomical structures of the embryo according to gestational age was detected in 6 (4.7%) pregnant women (Fig. 5, 6).
- A lag in the growth rate of the coccygeal-parietal size (CPD) was detected in 4 (3.1%) pregnant women. Normally, from 8 weeks of pregnancy, the increase in CTE is 10-12 mm per week.
Rice. 4.
Retrochorial hematoma.
A)
With signs of organization.
b)
No signs of organization.
Rice. 5.
Pregnancy 12 weeks. Gastroschisis (impaired differentiation of the main anatomical structures of the embryo).
Rice. 6.
Pregnancy 13 weeks. Omphalocele (impaired differentiation of the main anatomical structures of the embryo).
Sonographic signs of pathology of the uterus and ovaries
- Local thickening of the myometrium (hypertonicity) was detected in 100 (78.1%) pregnant women of the main group.
- The absence of corpus luteum cysts in the ovaries was detected in 74 (57.8%) pregnant women.
- The size of the adnexal mass exceeding 70 mm was diagnosed in 5 (3.9%) pregnant women. The factor of mechanical compression of the uterus, leading to hypertonicity of the myometrium, is important.
Doppler criteria for miscarriage were considered in isolation:
- Dissociated blood flow in the uterine arteries occurred in 40 (31.3%) pregnant women. The difference in systolic-diastolic ratio (SDR) in the right and left uterine arteries was 10-12% or 0.5 conventional units.
- Color Doppler mapping (CDC) revealed the absence of trophoblastic blood flow or intermittent vascularization (i.e., individual color loci in the chorion structure) in 3 (2.3%) pregnant women.
Discussion
Our study made it possible to establish that if pregnant women with threatened spontaneous miscarriage had three or more ultrasound “markers” of miscarriage in the first trimester, spontaneous miscarriage before 12 weeks occurred in 15 (11.7%) cases, late spontaneous miscarriage from 13 to 22 week in 7 (5.5%) cases and premature birth in 8 (6.25%) women.
It should be noted that in the presence of one or two echographic markers, not in all cases there were pronounced clinical symptoms of threatening spontaneous miscarriage. Thus, out of 100 (78.1%) pregnant women with ultrasound signs of myometrial hypertonicity and 74 (57.8%) with the absence of a corpus luteum cyst, only 30 (23.4%) pregnant women had reliable clinical signs. At the same time, all pregnant women who had echographic markers of pathology of extraembryonic structures, markers of pathology of the embryo and ovum were at high risk of developing spontaneous miscarriage and premature birth.
The validity of one or another echographic criterion determines the degree of accuracy of the prediction of miscarriage in the first trimester, and from a practical point of view, it is necessary to know how objectively this sign will allow one to predict spontaneous termination of pregnancy. The practical applicability of the criteria depends on their sensitivity and specificity. Sensitivity is the proportion of women in whom these echographic criteria were identified and the pregnancy ended in spontaneous termination, i.e. number of true positives. Specificity is the proportion of women in whom these signs were not established and pregnancy progressed, i.e. the number of true negative results (table).
Table
. Sensitivity and specificity of the main echographic criteria for miscarriage in the first trimester.
| Criterion | Sensitivity, % | Specificity, % |
| Amnion hypoplasia | 100 | 96 |
| Chorionic hypoplasia | 100 | 82 |
| Absence of corpus luteum in the ovaries | 54,3 | 77 |
| Impaired differentiation of the main structures of the embryo | 100 | 90 |
| Myometrial hypertonicity | 46,7 | 69 |
| Combination of 5 signs | 100 | 100 |
Thus, in the diagnosis of miscarriage using transvaginal echography, the most significant for predicting the outcome of this pregnancy are echographic markers of pathology of the embryo and extraembryonic structures, and the presence of ultrasound signs of pathology of the uterus and ovaries does not always lead to an unfavorable outcome of pregnancy.
Literature
- Sidelnikova V.M. Current problems of miscarriage. Clinical lectures. - M., 1999.
- Sidelnikova V.M. Miscarriage. - M.: Medicine, 1986.
- Ailamazyan E.K. Obstetrics: Textbook. manual for university students. - L., 1996, 250 p.
- Demidov V.N., Stygar A.M. Clinical significance of echography in early pregnancy //Akush. and gin. - 1985. - N 10. - P. 63-67.
- Mitkov V.V. Clinical guidelines for ultrasound diagnostics. - M.: 1996. T. 2. - P. 9 - 78.
- Persianinov L.S., Demidov V.N. Ultrasound diagnostics in obstetrics //Atlas. - M.: Medicine, 1982. - P. 336.
Accuvix-A30
Time-tested!
Ultrasound system for conducting examinations with expert diagnostic accuracy.
What is chorionic presentation and why does it occur?
Until the placenta is formed, the embryo is surrounded by a villous membrane, which grows into the lining of the uterus. Until the 16th week of gestation, this is the chorion (from the 17th week - the placenta), which performs the following main functions:
- Nutrition of the embryo;
- Respiration - delivery of oxygen and removal of carbon dioxide;
- Isolation of metabolic products;
- Embryo protection.
During the normal course of pregnancy, the chorion attaches to the fundus of the uterus and grows along the anterior, posterior and lateral walls, but this does not always happen.
Chorionic presentation is its incorrect location, in which there is complete or partial overlap of the internal os of the cervical canal.
Why this condition occurs is not completely clear. But a connection has been established with some factors:
- chronic inflammation of the uterus;
- previous operations;
- abnormal development of the uterus;
- a large number of pregnancies and births;
- low attachment of the placenta in the previous pregnancy.
Types of chorion location
Based on the attachment of the chorion relative to the internal os, presentation occurs:
- Complete - a condition in which the chorion completely covers the internal os. This will subsequently develop into placenta previa.
- Incomplete - characterized by overlap of part of the uterine os. If the villous membrane comes out up to a third, then this is called marginal presentation.
- Low - the chorion is located at a distance of 3 cm or less from the pharynx, but does not overlap it.
Chorionic presentation at 12 weeks is not the final verdict. As the uterus and fetus grow, migration may occur, and the condition will return to normal. A more favorable prognosis is noted for the posterior location of the chorion and presentation along the anterior wall.
Complete blocking of the uterine pharynx by the chorion is a dangerous type of pathology that threatens massive bleeding.
How is chorionic presentation manifested?
Most often, pathology is detected during ultrasound.
Bloody discharge can also be caused by presentation, especially if a hot bath, sauna, or sexual intercourse took place shortly before. In this case, you need to urgently consult a doctor.
Complications
The pathology is dangerous:
- premature miscarriage;
- uterine bleeding;
- intrauterine death of a child.
Chronic blood loss leads to the development of anemia and fetal hypoxia. If complete occlusion of the pharynx remains, natural childbirth is impossible.
Treatment of chorionic presentation
Partial chorionic presentation without bleeding does not require hospitalization. Isolation of any amount of blood is an indication for treatment in the hospital.
It is impossible to artificially change the location of the villous membrane, so the main task facing doctors is maintaining pregnancy. A protective treatment regime is created in the hospital:
- The woman is in a calm environment, on bed rest;
- Physical activity is limited;
- A balanced diet is provided with the exception of foods that strengthen or relax the stool.
Drug treatment is as follows:
- Suppositories with Papaverine, Drotaverine tablets to relieve uterine tone;
- Iron preparations, for example, Totema, Maltofer - for the prevention or treatment of anemia.
In the presence of bleeding, the hemostatic drug sodium etamsylate is additionally used. At the beginning of therapy, it is administered intravenously or intramuscularly. Then you can switch to tablets.
Massive bleeding that cannot be treated with conservative methods is an indication for termination of pregnancy.
After discharge from the hospital, at home it is necessary to adhere to a measured lifestyle, eliminate stress and increased workload. It is forbidden to have sex, because this may cause new bleeding and miscarriage.
What is the prognosis for the pathology?
Chorionic presentation at 8-14 weeks can transform into a normal location of the placenta or persist in the form of low placentation.
If the presentation does not disappear, but turns into an anomaly in the location of the placenta, then by the time of birth the baby may be transverse in the uterus or with the buttocks down. In such cases, to reduce the risk, it is recommended to deliver the baby through.
Prevention
Women should take care of their reproductive health as early as possible:
- Hypothermia should be avoided and inflammatory diseases of the genital area should be treated promptly.
- Do not resort to abortion, this is not a method of family planning.
- It is important to eat properly and nutritiously and lead a measured lifestyle.
If you follow these simple rules, you won’t have to become familiar with pathologies from personal experience.
Yulia Shevchenko, obstetrician-gynecologist, especially for the site
Ring-shaped placenta
Ultrasound scanner HS70
Accurate and confident diagnosis.
Multifunctional ultrasound system for conducting studies with expert diagnostic accuracy.
Introduction
Ring-shaped placenta (lat. placenta membranacea, or placenta diffusa) is a very rare anomaly of placental development, in which all or almost all fetal membranes remain covered with chorion villi, since there is no differentiation of the chorion into chorion leave and chorion frondosum [1]. The frequency of this pathology is 1:20,000-40,000 births [2]. The chorion begins to form from the 7-9th day of development of the fertilized egg. It remains ring-shaped until 7-8 weeks of pregnancy, then normally it is divided into smooth and branched. The ring-shaped placenta is characterized by an excessively large attachment area [3], while its thickness, even at the end of pregnancy, may not exceed 10 mm.
This anomaly is often accompanied by placenta accreta or placenta accreta, as well as umbilical cord vasa previa [4].
The course of pregnancy is complicated by repeated bleeding [5], late spontaneous miscarriages, premature birth, intrauterine growth retardation and fetal death [6]. And delivery is often complicated by postpartum hemorrhage and retention of placental tissue in the uterine cavity [1].
Material and methods
We present two cases of diagnosis of annular placenta and one case of annular chorion. Ultrasound studies were carried out on SonoAce-9900 scanners using a 3D 4-8ET/40/84 volumetric sensor and SonoAce-X8 using a 4-8 MHz volumetric sensor and Voluson E8.
results
Clinical observation 1
Pregnant D., 32 years old. This is the fourth pregnancy. The first and second ended in spontaneous miscarriages at 7-8 weeks. The third pregnancy ended in urgent birth, without any special features. This pregnancy proceeded with repeated hospitalizations for threatening miscarriage, accompanied by bloody discharge from the genital tract at 8-9 and 12-14 weeks, and threatening late miscarriage, marginal placenta previa at 21-22 weeks. The following data on the ultrasound examinations performed are known from the anamnesis.
At 17 weeks 5 days, fetometric indicators correspond to the period, no congenital malformation was detected. The placenta is located on the anterior wall of the uterus, thickness - 20 mm. At 24 weeks 6 days, fetometric indicators correspond to 26 weeks 5 days, no congenital malformation was detected. The placenta is located on the anterior wall, overlaps the internal os by 15 mm, thickness - 26 mm. At 28 weeks, fetometric indicators correspond to 30 weeks 5 days, no congenital malformation was detected. The placenta is located on the anterior wall, 33 mm above the edge of the internal os, thickness - 30 mm.
She was admitted to the hospital at 33-34 weeks of pregnancy with complaints of nagging pain in the lower abdomen. Ultrasound examination: pregnancy 33 weeks 4 days (fetometric indicators correspond to 35 weeks 6 days), no congenital malformation was detected. The placenta is located along the anterior, right and left side walls with a transition to the posterior wall (Fig. 1), lining the bottom, 17 mm above the edge of the internal os; the maximum thickness of the placenta is 18 mm (Fig. 2). An incomplete septum is defined above the internal pharynx (Fig. 3). Conclusion: “ring-shaped placenta.”
Rice. 1.
The placenta lines the anterior, right and left side walls of the uterus with a transition to the posterior wall.
Rice. 2.
Multiplanar 3D reconstruction mode. The placenta lines the anterior, right and left side walls of the uterus with a transition to the posterior wall. The arrow points to the septum in the uterine cavity.
Rice. 3.
Placenta at the site of insertion of the umbilical cord.
The next day, an emergency cesarean section was performed due to premature abruption of the low-lying placenta. The operation was accompanied by increased blood loss, which required surgical devascularization of the ascending branches of the a.uterinae on both sides. A child weighing 2500 g, length 45 cm with an Apgar score of 6/8 points was placed on mechanical ventilation an hour later. On the third day he was transferred to the premature ward.
Clinical observation 2
Pregnant A., 23 years old, first real pregnancy. She was admitted to the hospital with complaints of bloody discharge from the genital tract at 21-22 weeks of pregnancy. When conducting an ultrasound examination, the following data were obtained: fetometric indicators correspond to the period of 20-21 weeks, no congenital malformation was detected. The placenta is located along the anterior, right and left side walls with a transition to the posterior wall, lining the bottom, 10 mm above the edge of the internal pharynx; the maximum thickness in the area of umbilical cord attachment is 11 mm (Fig. 4). Above the internal os, a marginal placental abruption is detected with an area of detachment of the membranes 15x18 mm, up to 5 mm thick, with heterogeneous liquid contents (Fig. 5). Conclusion: “ring-shaped placenta, marginal placental abruption with detachment of membranes.” Therapy to maintain pregnancy was prescribed. The patient did not follow the instructions and left the hospital without permission.
Rice. 4.
The placenta lines the anterior, right and left side walls of the uterus with a transition to the posterior wall.
Rice. 5.
Placenta at the site of insertion of the umbilical cord.
Subsequently, according to the woman, at 28 weeks of pregnancy, repeated bleeding began and premature birth occurred. The child died on the first day.
Clinical observation 3
Pregnant Ts., 22 years old, first real pregnancy. I applied for an ultrasound examination at 12 weeks of pregnancy. The embryo corresponded to a period of 11 weeks 3 days; no CA markers were detected. The chorion lines all the walls and covers the internal os. The thickness of the chorion is from 15 to 20 mm (Fig. 6, 7). Conclusion: “Pregnancy 12 weeks. Ring-shaped chorion." An ultrasound examination is recommended at 16 weeks. During the study at 16 weeks, the placenta was located along the anterior wall, 18 mm thick. Subsequent studies revealed no pathology in the fetus or placenta. The pregnancy ended with an urgent birth of a full-term fetus.
Rice. 6.
The chorion lines all the walls of the uterus.
Rice. 7.
3D reconstruction mode. The chorion lines all the walls of the uterus.
Discussion
Having encountered the ring-shaped placenta for the first time, we turned to literature data. The information received turned out to be very little, and it was quite contradictory. In the first two cases, the course of pregnancy was accompanied by repeated bleeding, which led to premature birth and the death of the child on the first day in one of them. In the obstetric literature, in the sections on the causes of bleeding during pregnancy and premature birth, there is not a word about the ring-shaped placenta. CG Kaplan in his book “Color Atlas of Gross Placental Pathology” devotes only a few lines to this pathology, believing that an annular placenta has no clinical significance [7]. We searched MEDLINE using PabMed for all English-language articles published up to 2020 for the following terms: placenta membranacea, placenta diffusa. Only 20 references to articles mentioning this pathology were found. All articles describing cases of diagnosis of annular placenta spoke about various complications that accompanied this developmental anomaly.
Antepartum and postpartum hemorrhage complicated the course of pregnancy in 83 and 50% of cases, respectively [2]. According to the literature [1], pregnancy ended with hysterectomy in 28% of cases of annular placenta, and according to the authors [8], 30% of cases of placenta membranacea were accompanied by various anomalies of placenta attachment, up to placenta percreta.
From the first observation, it is clear that most prenatal ultrasound specialists were not prepared to encounter an annular placenta, despite the fact that modern ultrasound literature contains a description of this pathology [9, 10]. The patient underwent ultrasound examinations several times in various institutions and with different doctors. Attention was paid only to the location of the placenta relative to the internal os, and the fact that it lined almost the entire uterine cavity was left without attention, just as the thickness of the placenta was measured erroneously. Obstetricians and gynecologists were also not familiar with this anomaly of placental development and its possible complications.
In the second observation, a ring-shaped placenta was diagnosed at 21-22 weeks of pregnancy. But in this situation, the patient herself reacted to her diagnosis without proper understanding, which may have led to the death of the fetus.
We presented the third observation in order to show the possibility of diagnosing an annular placenta already during the first ultrasound examination. As mentioned above, the ring-shaped chorion remains normal until 7-8 weeks of pregnancy. In our case, there was a delay in the differentiation of the chorion: it remained ring-shaped even at 11-12 weeks. The pregnancy proceeded without complications.
Conclusion
Early identification of risk factors for obstetric hemorrhage is vital to improve maternal mortality and morbidity rates. These cases highlight the need for medical personnel, particularly ultrasound physicians, to be prepared to diagnose such a rare and unusual pathology as annular placenta.
Literature
- Ekoukou D., Ng Wing Tin L., Nere MB, Bourdet O., Elalaoui Y., Bazin C. Placenta membranacea. Review of the literature, a case report // J. Gynecol. Obstet. Biol. Reprod. (Paris). 1995; 24 (2): 189-93.
- Greenberg JA, Sorem KA, Shifren JL, Riley LE Placenta membranacea with placenta increta: a case report and literature review // Obstet Gynecol. 1991 Sep; 78 (3 Pt 2): 512-4.
- Molloy CE, McDowell W., Armor T., Crawford W., Bernstine R. Ultrasonic diagnosis of placenta membranacea in utero // J. Ultrasound. Med. 1983 Aug; 2 (8): 377-9.
- Dinh TV, Bedi DG, Salinas J. Placenta membranacea, previa and accreta. A case report // J. Reprod. Med. 1992 Jan; 37 (1): 97-9.
- Heras JL, Harding PG, Haust MD Recurrent bleeding associated with placenta membranacea partialis: report of a case // Am. J. Obstet. Gynecol. 1982 Oct 15; 144 (4): 480-2.
- Wilkins BS, Batcup G., Vinall PS Partial placenta membranacea // Br. J. Obstet. Gynaecol. July 1991; 98 (7): 675-9.
- Kaplan CG Color Atlas of Gross Placental Pathology (2-ed., Springer) 2007; 139-28.
- Sparic R., Kadija S., Tadic J., Dokic M., Milenkovic V. Intrapartal resection of the bicornuete uterus for placenta membranacea percreta // Srp. Arh. Celok. Lek. 2007 Jan-Feb; 135 (1-2): 85-7.
- Prenatal echography. Ed. Medvedeva M.V. Moscow: Real Time, 2005. 560 p.
- Ultrasound diagnostics in obstetrics and gynecology. Ed. Volkova A.E. Rostov-on-Don: Phoenix, 2006. 480 p.
Ultrasound scanner HS70
Accurate and confident diagnosis.
Multifunctional ultrasound system for conducting studies with expert diagnostic accuracy.